Thorne Carter, Boire Gilles, Chow Andrew, Garces Kirsten, Liu Fang, Poulin-Costello Melanie, Walker Valery, Haraoui Boulos
The Arthritis Program Research Group, Southlake Regional Health Centre, c/o 43 Lundy's Lane, Newmarket, ON, L3Y 3R7, Canada.
Centre Hospitalier Universitaire de Sherbrooke (CIUSSS de l'Estrie-CHUS), Université de Sherbrooke, Sherbrooke, QC, Canada.
Open Rheumatol J. 2017 Oct 24;11:123-135. doi: 10.2174/1874312901711010123. eCollection 2017.
To compare anti-TNF dose escalation, DMARD and/or glucocorticoid intensification, switches to another biologic, and drug and drug-related costs over 12 and 18 months for rheumatoid arthritis (RA) patients initiating etanercept (ETN), adalimumab (ADA), or infliximab (IFX) in routine clinical practice across Canada.
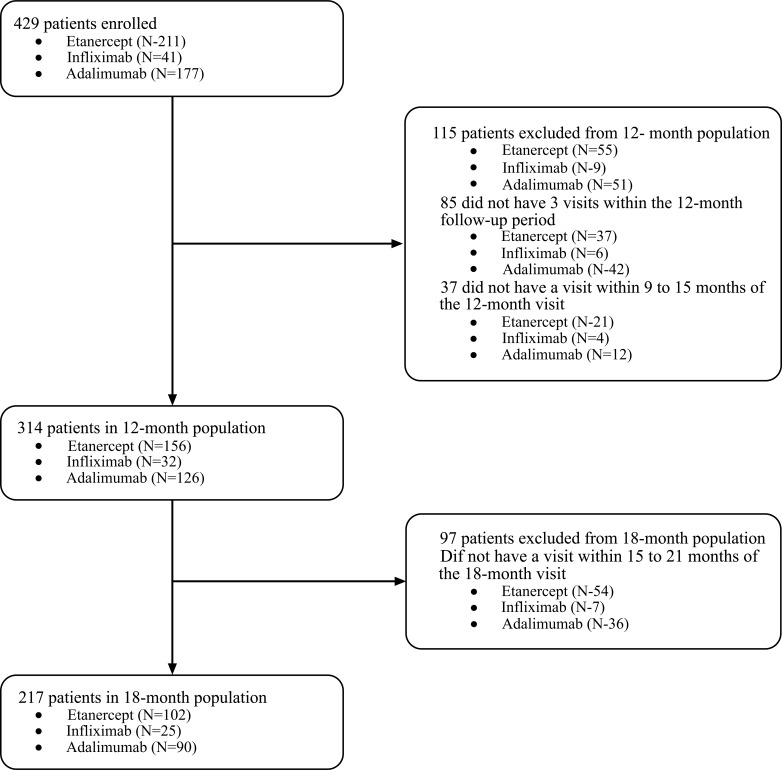
A retrospective chart review of biologic-naïve adult RA patients newly initiating ADA, ETN, or IFX between January 01, 2006 and December 31, 2012 from 11 practices across Canada.
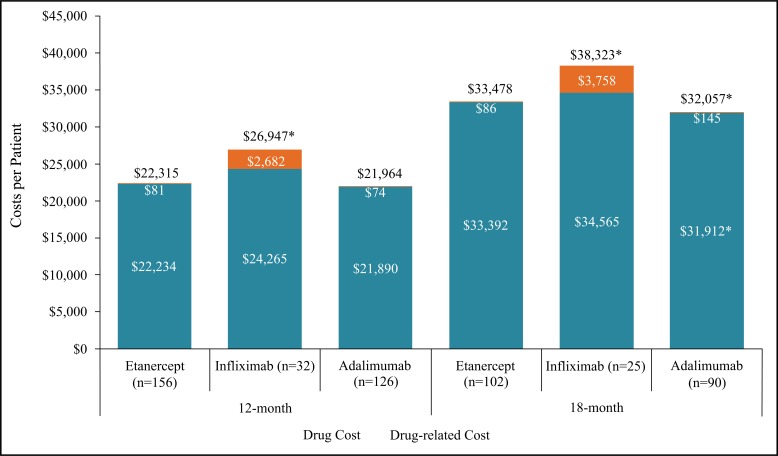
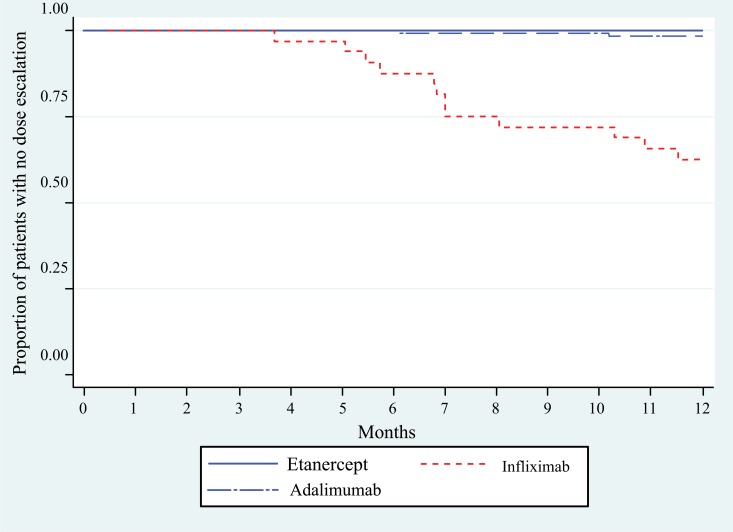
There were 314 patients in the 12-month analysis and 217 in the 18-month analysis. No dose escalation occurred with ETN over 12 and 18 months versus 38% and 32% for IFX (p<0.001) and 2% and 2% for ADA (p=0.199, p=0.218). Over 18 months, dose escalation and/or DMARD and/or glucocorticoid intensification was less frequent among ETN (16%) versus IFX (44%, p=0.005) and ADA (34%, p=0.004). By 18 months, 22% of patients initiating ADA had switched to another biologic compared with 6% of ETN patients (p=0.001).Patients initiating ETN had lower total (drug and drug-related) costs over 12 and 18 months compared to IFX, and no difference compared to ADA when adjusted for potential confounders. Patients with dose escalation had higher costs compared to those with no dose escalation.
Physicians were more likely to escalate the dose of IFX, but optimize co-therapy with ADA and ETN. ETN patients had no dose escalation and were less likely to have DMARD and/or glucocorticoid intensification than ADA patients. ETN-treated patients had lower costs compared to IFX patients.
比较在加拿大常规临床实践中,开始使用依那西普(ETN)、阿达木单抗(ADA)或英夫利昔单抗(IFX)的类风湿关节炎(RA)患者在12个月和18个月内抗TNF剂量增加、改善病情抗风湿药(DMARD)和/或糖皮质激素强化、换用另一种生物制剂以及药物和药物相关成本的情况。
对2006年1月1日至2012年12月31日期间加拿大11家医疗机构中初治的成年RA患者进行回顾性病历审查,这些患者新开始使用ADA、ETN或IFX。
12个月分析中有314例患者,18个月分析中有217例患者。ETN在12个月和18个月内均未出现剂量增加,而IFX分别为38%和32%(p<0.001),ADA分别为2%和2%(p=0.199,p=0.218)。在18个月期间,ETN患者中剂量增加和/或DMARD和/或糖皮质激素强化的频率低于IFX(44%,p=0.005)和ADA(34%,p=0.004)。到18个月时,开始使用ADA的患者中有22%换用了另一种生物制剂,而开始使用ETN的患者中这一比例为6%(p=0.001)。与IFX相比,开始使用ETN的患者在12个月和18个月内的总(药物和药物相关)成本更低,在调整潜在混杂因素后与ADA相比无差异。剂量增加的患者成本高于未增加剂量的患者。
医生更倾向于增加IFX的剂量,但会优化ADA和ETN的联合治疗。与ADA患者相比,ETN患者未出现剂量增加,且DMARD和/或糖皮质激素强化的可能性较小。与IFX治疗的患者相比,ETN治疗的患者成本更低。