Kunert A, Chmielewski M, Wijers R, Berrevoets C, Abken H, Debets R
Laboratory of Tumor Immunology, Department of Medical Oncology, Erasmus MC Cancer Institute, Rotterdam, The Netherlands.
Department I of Internal Medicine, University Hospital Cologne and Center for Molecular Medicine Cologne, University of Cologne, Cologne, Germany.
Oncoimmunology. 2017 Oct 11;7(1):e1378842. doi: 10.1080/2162402X.2017.1378842. eCollection 2017.
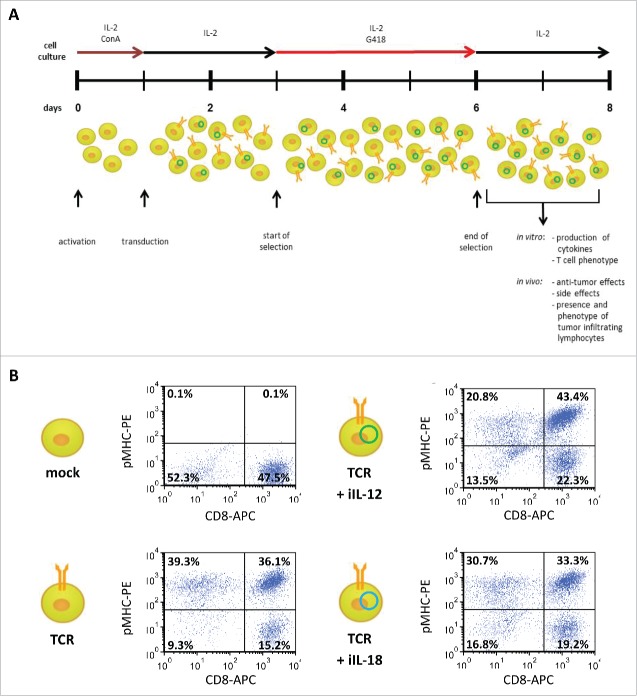
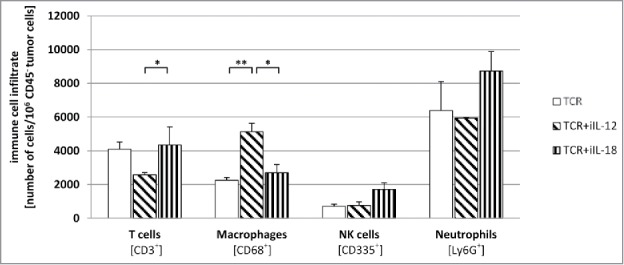
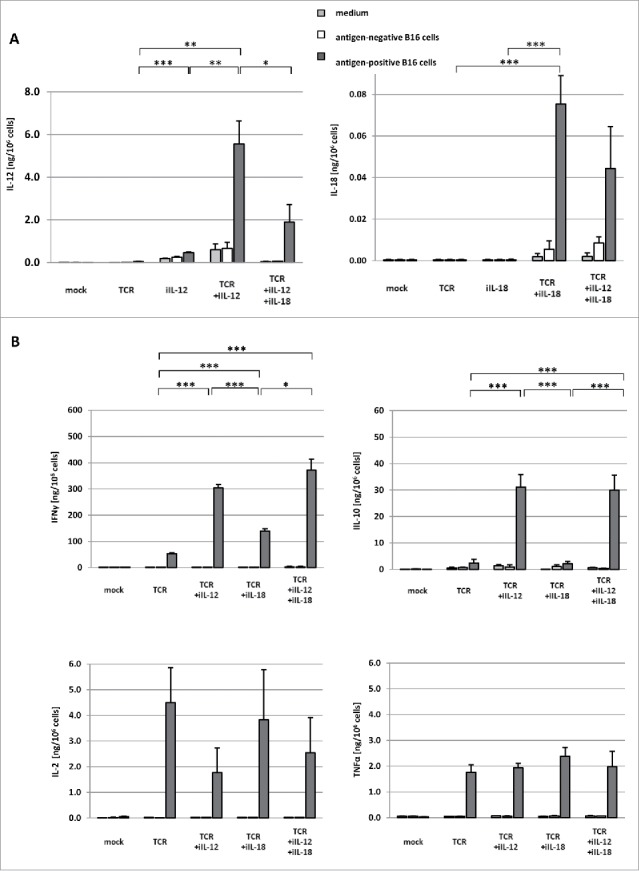
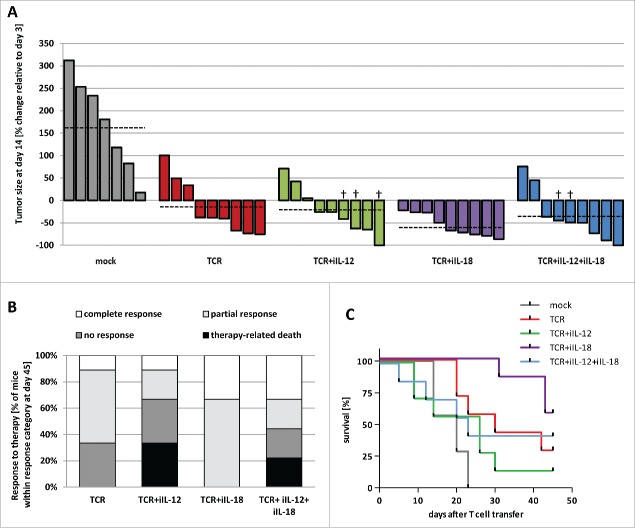
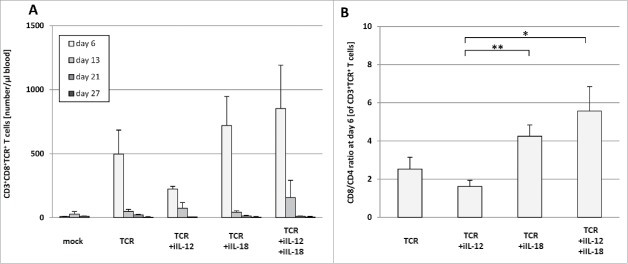
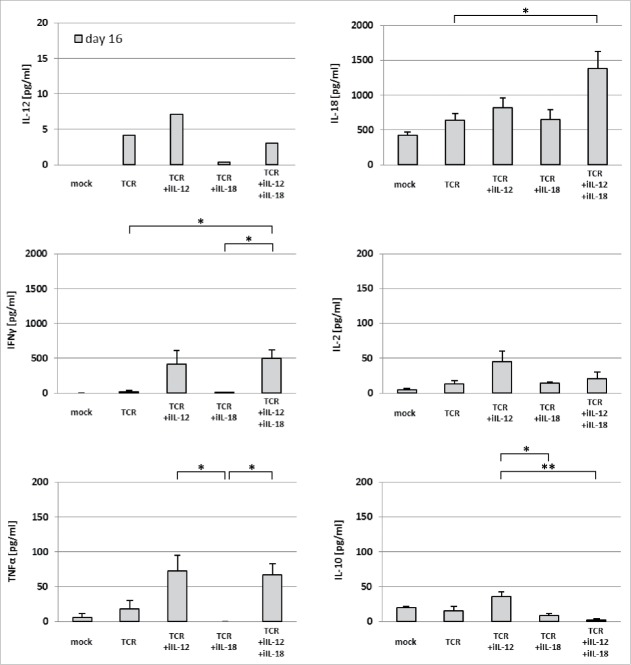
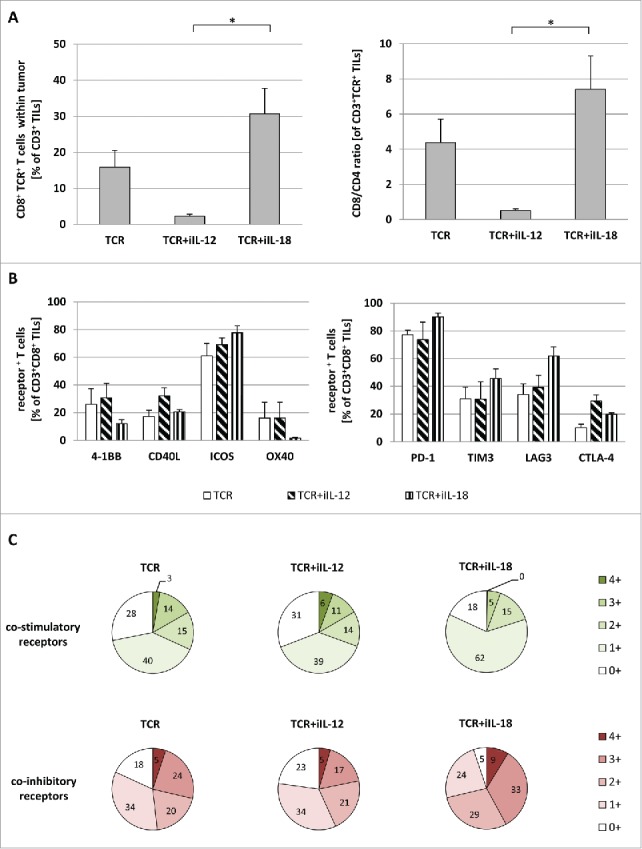
Adoptive therapy with engineered T cells shows promising results in treating patients with malignant disease, but is challenged by incomplete responses and tumor recurrences. Here, we aimed to direct the tumor microenvironment in favor of a successful immune response by local secretion of interleukin (IL-) 12 and IL-18 by sadministered T cells. To this end, we engineered T cells with a melanoma-specific T cell receptor (TCR) and murine IL-12 and/or IL-18 under the control of a nuclear-factor of activated T-cell (NFAT)-sensitive promoter. These T cells produced IL-12 or IL-18, and consequently enhanced levels of IFNγ, following exposure to antigen-positive but not negative tumor cells. Adoptive transfer of T cells with a TCR and inducible (i)IL-12 to melanoma-bearing mice resulted in severe, edema-like toxicity that was accompanied by enhanced levels of IFNγ and TNFα in blood, and reduced numbers of peripheral TCR transgene-positive T cells. In contrast, transfer of T cells expressing a TCR and iIL-18 was without side effects, enhanced the presence of therapeutic CD8 T cells within tumors, reduced tumor burden and prolonged survival. Notably, treatment with TCR+iIL-12 but not iIL-18 T cells resulted in enhanced intra-tumoral accumulation of macrophages, which was accompanied by a decreased frequency of therapeutic T cells, in particular of the CD8 subset. In addition, when administered to mice, iIL-18 but not iIL-12 demonstrated a favorable profile of T cell co-stimulatory and inhibitory receptors. In conclusion, we observed that treatment with T cells engineered with a TCR and iIL18 T cells is safe and able to skew the tumor microenvironment in favor of an improved anti-tumor T cell response.
经工程改造的T细胞过继性疗法在治疗恶性疾病患者方面显示出有前景的结果,但受到反应不完全和肿瘤复发的挑战。在此,我们旨在通过经给药的T细胞局部分泌白细胞介素(IL-)12和IL-18来引导肿瘤微环境,以利于成功的免疫反应。为此,我们用黑色素瘤特异性T细胞受体(TCR)以及在活化T细胞核因子(NFAT)敏感启动子控制下的小鼠IL-12和/或IL-18对T细胞进行工程改造。这些T细胞在暴露于抗原阳性而非阴性肿瘤细胞后产生IL-12或IL-18,并因此提高了IFNγ水平。将携带TCR和诱导型(i)IL-12的T细胞过继转移至荷黑色素瘤小鼠体内会导致严重的、类似水肿的毒性,伴有血液中IFNγ和TNFα水平升高以及外周TCR转基因阳性T细胞数量减少。相比之下,表达TCR和iIL-18的T细胞转移没有副作用,增加了肿瘤内治疗性CD8 T细胞的存在,减轻了肿瘤负担并延长了生存期。值得注意的是,用TCR+iIL-12而非iIL-18 T细胞治疗导致肿瘤内巨噬细胞积聚增加,同时治疗性T细胞,特别是CD8亚群的频率降低。此外,当给予小鼠时,iIL-18而非iIL-12表现出有利的T细胞共刺激和抑制受体谱。总之,我们观察到用TCR和iIL18 T细胞工程改造的T细胞进行治疗是安全的,并且能够使肿瘤微环境向有利于改善抗肿瘤T细胞反应的方向转变。