Miller Cecelia R, Ruppert Amy S, Heerema Nyla A, Maddocks Kami J, Labanowska Jadwiga, Breidenbach Heather, Lozanski Gerard, Zhao Weiqiang, Gordon Amber L, Jones Jeffrey A, Flynn Joseph M, Jaglowski Samantha M, Andritsos Leslie A, Blum Kristie A, T Awan Farrukh, Rogers Kerry A, Grever Michael R, Johnson Amy J, Abruzzo Lynne V, Hertlein Erin K, Blachly James S, Woyach Jennifer A, Byrd John C
Division of Hematology, Department of Internal Medicine.
Department of Pathology, and.
Blood Adv. 2017 Aug 21;1(19):1584-1588. doi: 10.1182/bloodadvances.2017007302. eCollection 2017 Aug 22.
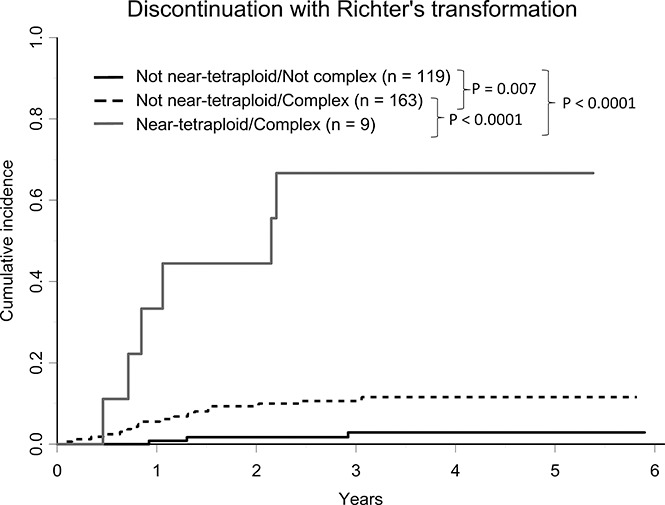
Ibrutinib is a highly effective targeted therapy for chronic lymphocytic leukemia (CLL). However, ibrutinib must be discontinued in a subset of patients due to progressive CLL or transformation to aggressive lymphoma (Richter transformation). Transformation occurs early in the course of therapy and has an extremely poor prognosis. Thus, identification of prognostic markers associated with transformation is of utmost importance. Near-tetraploidy (4 copies of most chromosomes within a cell) has been reported in various lymphomas, but its incidence and significance in CLL has not been described. Using fluorescence in situ hybridization, we detected near-tetraploidy in 9 of 297 patients with CLL prior to beginning ibrutinib treatment on 1 of 4 clinical trials (3.0%; 95% confidence interval [CI], 1.4%-5.7%). Near-tetraploidy was associated with aggressive disease characteristics: Rai stage 3/4 ( = .03), deletion 17p ( = .03), and complex karyotype ( = .01). Near-tetraploidy was also associated with ibrutinib discontinuation due to Richter transformation ( < .0001), but not due to progressive CLL ( = .41). Of the 9 patients with near-tetraploidy, 6 had Richter transformation with diffuse large B-cell lymphoma. In a multivariable model, near-tetraploidy (hazard ratio [HR], 8.66; 95% CI, 3.83-19.59; < .0001) and complex karyotype (HR, 4.77; 95% CI, 1.42-15.94; = .01) were independent risk factors for discontinuing ibrutinib due to transformation. Our results suggest that near-tetraploidy is a potential prognostic marker for Richter transformation to assess in patients going on ibrutinib.
依鲁替尼是治疗慢性淋巴细胞白血病(CLL)的一种高效靶向疗法。然而,由于CLL病情进展或转化为侵袭性淋巴瘤(里氏转化),部分患者必须停用依鲁替尼。转化发生在治疗早期,预后极差。因此,识别与转化相关的预后标志物至关重要。在各种淋巴瘤中均报道过近四倍体(细胞内大多数染色体有4条拷贝),但其在CLL中的发生率及意义尚未见描述。我们采用荧光原位杂交技术,在4项临床试验中的1项里,于297例接受依鲁替尼治疗前的CLL患者中检测到9例近四倍体(3.0%;95%置信区间[CI],1.4% - 5.7%)。近四倍体与侵袭性疾病特征相关:Rai分期3/4期(P = 0.03)、17p缺失(P = 0.03)和复杂核型(P = 0.01)。近四倍体还与因里氏转化而停用依鲁替尼相关(P < 0.0001),但与因CLL病情进展而停用无关(P = 0.41)。在9例近四倍体患者中,6例发生了伴有弥漫性大B细胞淋巴瘤的里氏转化。在多变量模型中,近四倍体(风险比[HR],8.66;95% CI,3.83 - 19.59;P < 0.0001)和复杂核型(HR,4.77;95% CI,1.42 - 15.94;P = 0.01)是因转化而停用依鲁替尼的独立危险因素。我们的结果表明,近四倍体是接受依鲁替尼治疗患者里氏转化的一个潜在预后标志物,值得评估。