Withers Barbara, Blyth Emily, Clancy Leighton E, Yong Agnes, Fraser Chris, Burgess Jane, Simms Renee, Brown Rebecca, Kliman David, Dubosq Ming-Celine, Bishop David, Sutrave Gaurav, Ma Chun Kei Kris, Shaw Peter J, Micklethwaite Kenneth P, Gottlieb David J
Westmead Institute for Medical Research, University of Sydney, Sydney, NSW, Australia.
Blood and Bone Marrow Transplant Unit.
Blood Adv. 2017 Nov 2;1(24):2193-2205. doi: 10.1182/bloodadvances.2017010223. eCollection 2017 Nov 14.
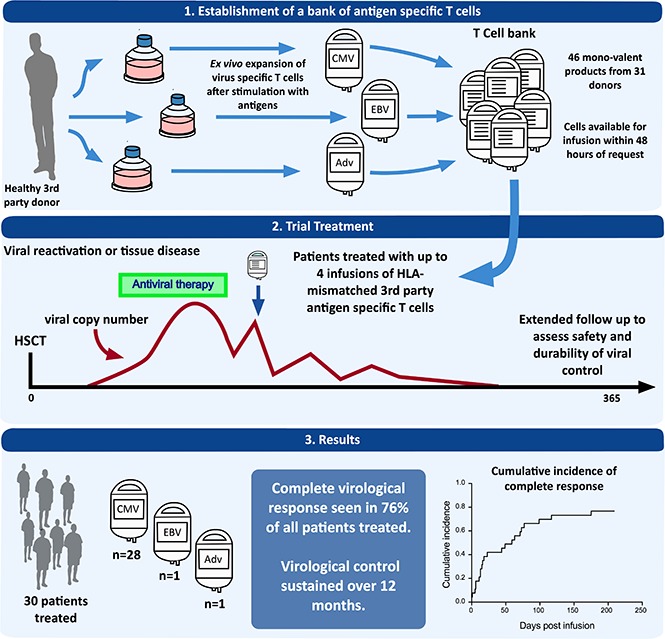
Donor-derived adoptive T-cell therapy is a safe and effective treatment of viral infection posttransplant, but it is limited by donor serostatus and availability and by its personalized nature. Off-the-shelf, third-party virus-specific T cells (VSTs) appear promising, but the long-term safety and durability of responses have yet to be established. We conducted a prospective study of 30 allogeneic hemopoietic stem cell transplant (HSCT) patients with persistent or recurrent cytomegalovirus (CMV) (n = 28), Epstein-Barr virus (n = 1), or adenovirus (n = 1) after standard therapy. Patients were treated with infusions of partially HLA-matched, third-party, ex vivo-expanded VSTs (total = 50 infusions) at a median of 75 days post-HSCT (range, 37 to 349 days). Safety, viral dynamics, and immune recovery were monitored for 12 months. Infusions were safe and well tolerated. Acute graft versus host disease occurred in 2 patients, despite a median HLA match between VSTs and the recipient of 2 of 6 antigens. At 12 months, the cumulative incidence of overall response was 93%. Virological control was durable in the majority of patients; the reintroduction of antiviral therapy after the final infusion occurred in 5 patients. CMV-specific T-cell immunity rose significantly and coincided with a rise in CD8 terminal effector cells. PD-1 expression was elevated on CD8 lymphocytes before the administration of third-party T cells and remained elevated at the time of viral control. Third-party VSTs show prolonged benefit, with virological control achieved in association with the recovery of CD8 effector T cells possibly facilitated by VST infusion. This trial was registered at www.clinicaltrials.gov as #NCT02779439 and www.anzctr.org.au as #ACTRN12613000603718.
供体来源的过继性T细胞疗法是一种安全有效的移植后病毒感染治疗方法,但它受到供体血清状态、可用性及其个性化性质的限制。现成的第三方病毒特异性T细胞(VST)似乎很有前景,但反应的长期安全性和持久性尚未确立。我们对30例接受标准治疗后仍有持续性或复发性巨细胞病毒(CMV)(n = 28)、爱泼斯坦-巴尔病毒(n = 1)或腺病毒(n = 1)感染的异基因造血干细胞移植(HSCT)患者进行了一项前瞻性研究。患者在HSCT后中位75天(范围37至349天)接受了部分HLA匹配的第三方体外扩增VST输注(共50次输注)。对安全性、病毒动态和免疫恢复进行了12个月的监测。输注是安全的且耐受性良好。2例患者发生了急性移植物抗宿主病,尽管VST与受体之间的HLA抗原匹配中位值为6个中的2个。12个月时,总体反应的累积发生率为93%。大多数患者的病毒学控制是持久的;最后一次输注后5例患者重新开始抗病毒治疗。CMV特异性T细胞免疫显著升高,与CD8终末效应细胞的升高同时出现。在给予第三方T细胞之前,CD8淋巴细胞上的PD-1表达升高,在病毒控制时仍保持升高。第三方VST显示出持久的益处,通过VST输注可能促进了CD8效应T细胞的恢复并实现了病毒学控制。该试验在www.clinicaltrials.gov上注册为#NCT02779439,在www.anzctr.org.au上注册为#ACTRN12613000603718。