Laboratory for Molecular Medicine, Partners Healthcare Personalized Medicine, Boston, Massachusetts, USA.
Stanford Center for Inherited Cardiovascular Disease, Stanford University, Stanford, California, USA.
Genet Med. 2018 Mar;20(3):351-359. doi: 10.1038/gim.2017.218. Epub 2018 Jan 4.
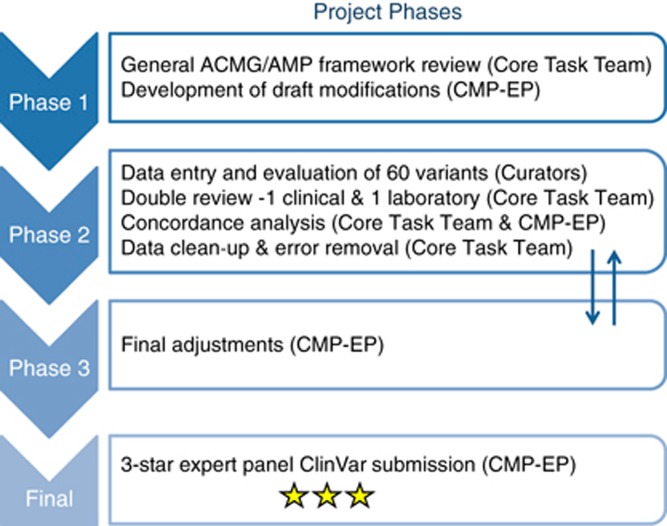
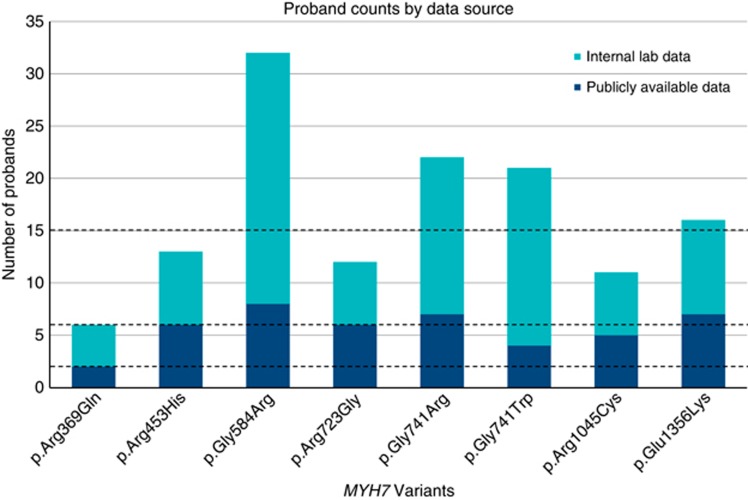
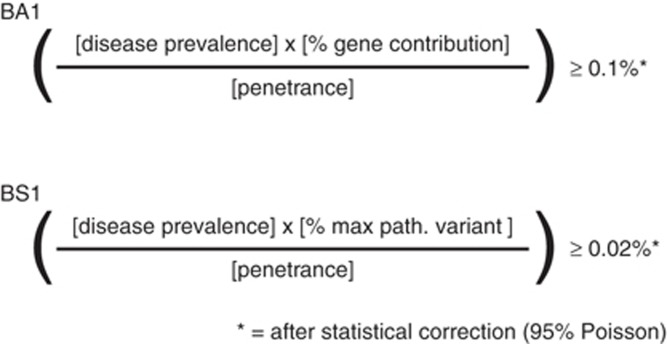
PurposeIntegrating genomic sequencing in clinical care requires standardization of variant interpretation practices. The Clinical Genome Resource has established expert panels to adapt the American College of Medical Genetics and Genomics/Association for Molecular Pathology classification framework for specific genes and diseases. The Cardiomyopathy Expert Panel selected MYH7, a key contributor to inherited cardiomyopathies, as a pilot gene to develop a broadly applicable approach.MethodsExpert revisions were tested with 60 variants using a structured double review by pairs of clinical and diagnostic laboratory experts. Final consensus rules were established via iterative discussions.ResultsAdjustments represented disease-/gene-informed specifications (12) or strength adjustments of existing rules (5). Nine rules were deemed not applicable. Key specifications included quantitative frameworks for minor allele frequency thresholds, the use of segregation data, and a semiquantitative approach to counting multiple independent variant occurrences where fully controlled case-control studies are lacking. Initial inter-expert classification concordance was 93%. Internal data from participating diagnostic laboratories changed the classification of 20% of the variants (n = 12), highlighting the critical importance of data sharing.ConclusionThese adapted rules provide increased specificity for use in MYH7-associated disorders in combination with expert review and clinical judgment and serve as a stepping stone for genes and disorders with similar genetic and clinical characteristics.
目的
将基因组测序整合到临床护理中需要标准化变异解释实践。临床基因组资源已经建立了专家小组,以适应美国医学遗传学和基因组学学院/分子病理学协会的分类框架,用于特定的基因和疾病。心肌病专家小组选择 MYH7(遗传性心肌病的关键贡献者)作为试点基因,以开发一种广泛适用的方法。
方法
使用由临床和诊断实验室专家组成的配对进行结构化的双次审查,对 60 个变体进行了专家修订测试。通过迭代讨论确定了最终的共识规则。
结果
调整代表疾病/基因信息的规范(12 个)或现有规则的强度调整(5 个)。有 9 条规则被认为不适用。关键规范包括次要等位基因频率阈值的定量框架、分离数据的使用以及在缺乏完全对照病例对照研究的情况下对多个独立变异发生进行半定量计数的方法。最初的专家间分类一致性为 93%。来自参与诊断实验室的内部数据改变了 20%的变体的分类(n=12),突出了数据共享的至关重要性。
结论
这些经过调整的规则为与专家审查和临床判断相结合使用 MYH7 相关疾病提供了更高的特异性,并为具有类似遗传和临床特征的基因和疾病提供了一个垫脚石。