Letourneau Lisa R, Carmody David, Philipson Louis H, Greeley Siri Atma W
Department of Medicine, Section of Adult and Pediatric Endocrinology, Diabetes and Metabolism, University of Chicago, Chicago, Illinois, 60637.
Department of Endocrinology, Singapore General Hospital, Singapore 169608.
J Endocr Soc. 2017 Nov 24;2(1):1-8. doi: 10.1210/js.2017-00356. eCollection 2018 Jan 1.
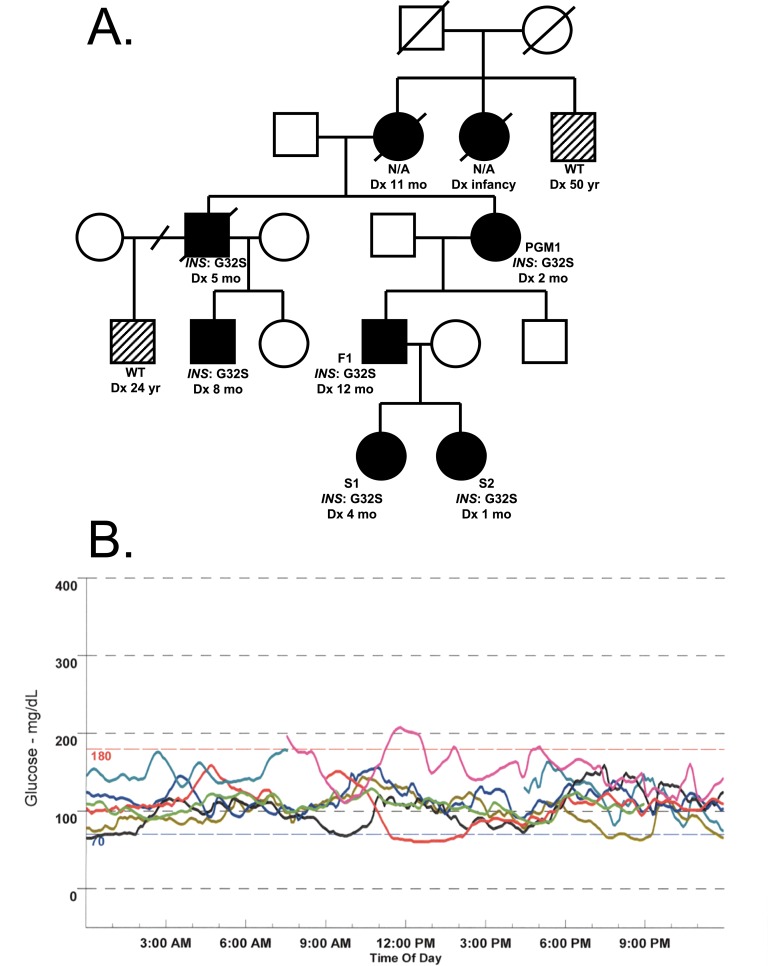
Although mutations in the proinsulin gene () are the second most common cause of neonatal diabetes mellitus, the natural history of -cell death and the most appropriate treatments remains unknown. We describe the management and outcome of two sisters with -mediated diabetes (S1 and S2) and suggest that more intensive insulin treatment of S2 may have resulted in better clinical outcomes. S1 was diagnosed with diabetes after presenting with serum glucose of 404 mg/dL (22.4 mmol/L) and started multiple daily insulin injections at age 4 months, followed by continuous subcutaneous insulin infusion (CSII) at age 42 months. S1 had positive genetic testing at age 4 months for the GlyB8Ser or Gly32Ser mutation in proinsulin. S2 had positive research-based genetic testing, age 1 month, before she had consistently elevated blood glucose levels. Continuous glucose monitoring revealed abnormal excursions to 200 mg/dL. Low-dose insulin therapy was initiated at age 2.5 months via CSII. At age-matched time points, S2 had higher C-peptide levels, lower hemoglobin A1c values, and lower estimated doses of insulin as compared with S1. Earlier, more intensive insulin treatment was associated with higher C-peptide levels, decreased insulin dosing, and improved glycemic control. Initiating exogenous insulin before overt hyperglycemia and maintaining intensive insulin management may reduce the demand for endogenous insulin production and may preserve -cell function. Studies accumulating data on greater numbers of participants will be essential to determine whether these associations are consistent for all gene mutations.
尽管胰岛素原基因()突变是新生儿糖尿病的第二大常见病因,但β细胞死亡的自然病程以及最恰当的治疗方法仍不明确。我们描述了两名患有β细胞介导糖尿病的姐妹(S1和S2)的治疗情况及预后,并指出对S2进行更强化的胰岛素治疗可能会带来更好的临床结果。S1在血糖达到404mg/dL(22.4mmol/L)后被诊断为糖尿病,4个月大时开始每日多次注射胰岛素,42个月大时改为持续皮下胰岛素输注(CSII)。S1在4个月大时胰岛素原基因的GlyB8Ser或Gly32Ser突变基因检测呈阳性。S2在1个月大时,在血糖持续升高之前,基于研究的基因检测呈阳性。持续血糖监测显示血糖异常波动至200mg/dL。2.5个月大时通过CSII开始低剂量胰岛素治疗。在年龄匹配的时间点,与S1相比,S2的C肽水平更高、糖化血红蛋白值更低、胰岛素估计剂量更低。更早、更强化的胰岛素治疗与更高的C肽水平、胰岛素剂量减少和血糖控制改善相关。在明显高血糖之前开始外源性胰岛素治疗并维持强化胰岛素管理,可能会减少内源性胰岛素产生的需求,并可能保留β细胞功能。积累更多参与者数据的研究对于确定这些关联是否适用于所有基因突变更为关键。