Nephrology Section, Department of Internal Medicine, Ghent University Hospital, De Pintelaan 185, 9000 Ghent, Belgium.
Toxins (Basel). 2018 Jan 8;10(1):33. doi: 10.3390/toxins10010033.
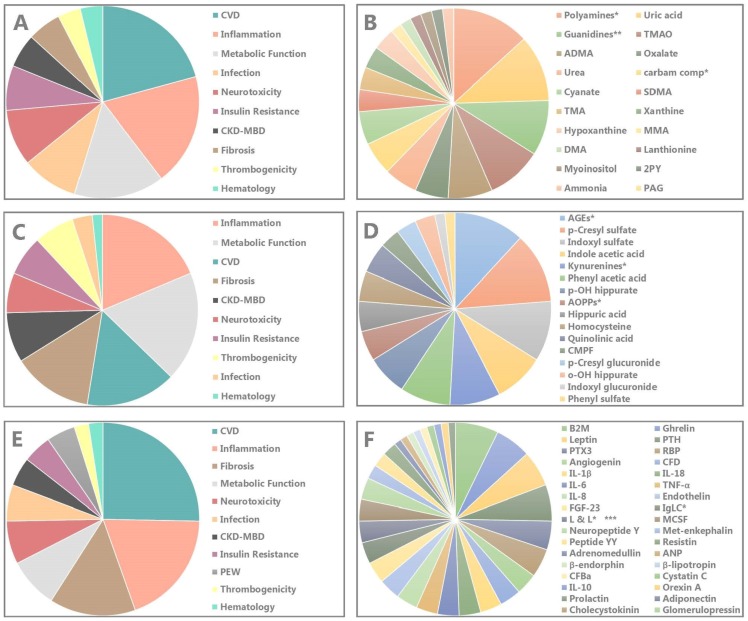
In this narrative review, the biological/biochemical impact (toxicity) of a large array of known individual uremic retention solutes and groups of solutes is summarized. We classified these compounds along their physico-chemical characteristics as small water-soluble compounds or groups, protein bound compounds and middle molecules. All but one solute (glomerulopressin) affected at least one mechanism with the potential to contribute to the uremic syndrome. In general, several mechanisms were influenced for each individual solute or group of solutes, with some impacting up to 7 different biological systems of the 11 considered. The inflammatory, cardio-vascular and fibrogenic systems were those most frequently affected and they are one by one major actors in the high morbidity and mortality of CKD but also the mechanisms that have most frequently been studied. A scoring system was built with the intention to classify the reviewed compounds according to the experimental evidence of their toxicity (number of systems affected) and overall experimental and clinical evidence. Among the highest globally scoring solutes were 3 small water-soluble compounds [asymmetric dimethylarginine (ADMA); trimethylamine-N-oxide (TMAO); uric acid], 6 protein bound compounds or groups of protein bound compounds [advanced glycation end products (AGEs); p-cresyl sulfate; indoxyl sulfate; indole acetic acid; the kynurenines; phenyl acetic acid;] and 3 middle molecules [β₂-microglobulin; ghrelin; parathyroid hormone). In general, more experimental data were provided for the protein bound molecules but for almost half of them clinical evidence was missing in spite of robust experimental data. The picture emanating is one of a complex disorder, where multiple factors contribute to a multisystem complication profile, so that it seems of not much use to pursue a decrease of concentration of a single compound.
在这篇叙述性评论中,总结了大量已知的个体尿毒症潴留溶质和溶质组的生物/生化影响(毒性)。我们根据物理化学特性将这些化合物分类为小的水溶性化合物或化合物组、与蛋白质结合的化合物和中分子。除了一种溶质(肾小球加压素)外,所有溶质至少影响了一种可能导致尿毒症综合征的机制。一般来说,每种单独的溶质或溶质组都会影响几种机制,其中一些会影响到 11 个考虑因素中的 7 个不同的生物系统。炎症、心血管和纤维生成系统是受影响最频繁的系统,它们是 CKD 高发病率和高死亡率的主要因素,也是最常被研究的机制。建立了一个评分系统,旨在根据毒性的实验证据(受影响的系统数量)以及总体实验和临床证据对所审查的化合物进行分类。在全球范围内得分最高的溶质包括 3 种小的水溶性化合物[不对称二甲基精氨酸(ADMA);三甲胺 N-氧化物(TMAO);尿酸]、6 种与蛋白质结合的化合物或与蛋白质结合的化合物组[晚期糖基化终产物(AGEs);对甲酚硫酸盐;吲哚硫酸盐;吲哚乙酸;色氨酸;苯乙酸]和 3 种中分子[β₂-微球蛋白;胃饥饿素;甲状旁腺激素)。一般来说,与蛋白质结合的分子提供了更多的实验数据,但其中近一半缺乏临床证据,尽管有可靠的实验数据。由此产生的情况是一种复杂的疾病,多种因素导致多系统并发症,因此,追求单一化合物浓度的降低似乎没有多大用处。