Konda Sanjit R, Lott Ariana, Saleh Hesham, Schubl Sebastian, Chan Jeffrey, Egol Kenneth A
Department of Orthopedic Surgery, NYU Langone Orthopedic Hospital, New York, NY, USA.
Jamaica Hospital Medical Center, New York, NY, USA.
Geriatr Orthop Surg Rehabil. 2017 Dec;8(4):225-230. doi: 10.1177/2151458517735202. Epub 2017 Oct 25.
Frailty in elderly trauma populations has been correlated with an increased risk of morbidity and mortality. The Score for Trauma Triage in the Geriatric and Middle-Aged (STTGMA) is a validated mortality risk score that evaluates 4 major physiologic criteria: age, comorbidities, vital signs, and anatomic injuries. The aim of this study was to investigate whether the addition of additional frailty variables to the STTGMA tool would improve risk stratification of a middle-aged and elderly trauma population.
A total of 1486 patients aged 55 years and older who met the American College of Surgeons Tier 1 to 3 criteria and/or who had orthopedic or neurosurgical traumatic consultations in the emergency department between September 2014 and September 2016 were included. The STTGMA and STTGMA scores were calculated. Additional "frailty variables" included preinjury assistive device use (disability), independent ambulatory status (functional independence), and albumin level (nutrition). The ability of the STTGMA and the STTGMA models to predict inpatient mortality was compared using area under the receiver operating characteristic curves (AUROCs).
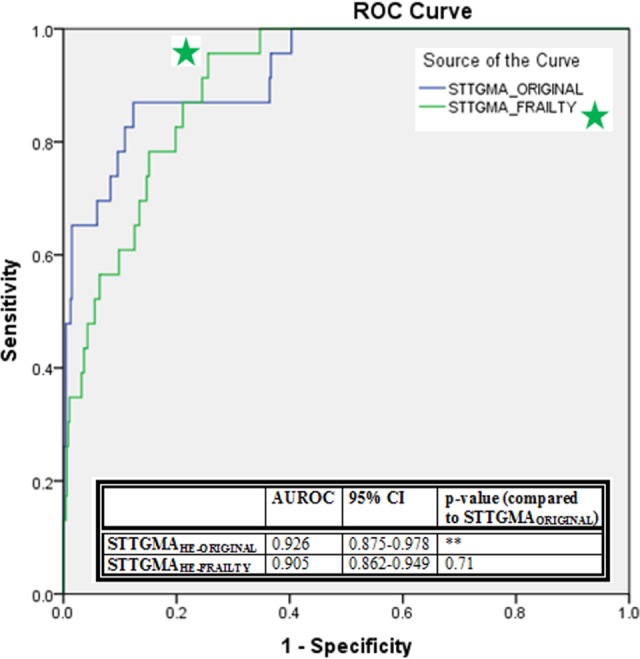
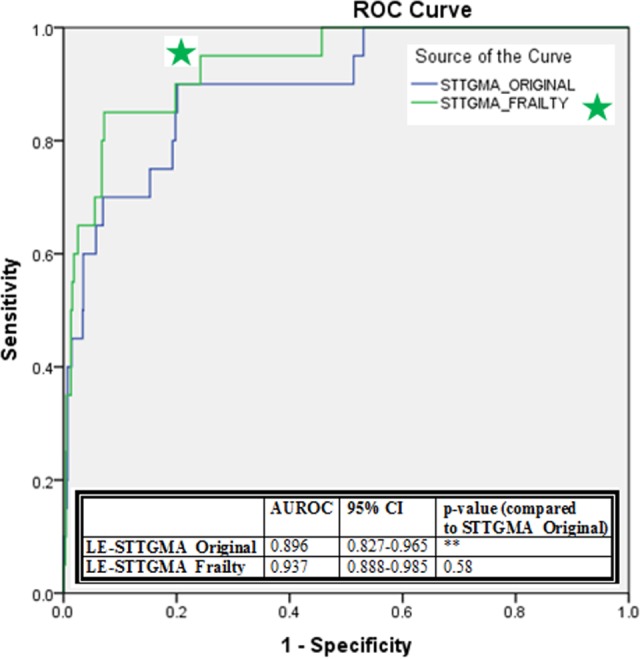
There were 23 high-energy inpatient mortalities (4.7%) and 20 low-energy inpatient mortalities (2.0%). When the STTGMA model was used, the AUROC in the high-energy and low-energy cohorts was 0.926 and 0.896, respectively. The AUROC for STTGMA for the high-energy and low-energy cohorts was 0.905 and 0.937, respectively. There was no significant difference in predictive capacity for inpatient mortality between STTGMA and STTGMA for both the high-energy and low-energy cohorts.
The original STTGMA tool accounts for important frailty factors including cognition and general health status. These variables combined with other major physiologic variables such as age and anatomic injuries appear to be sufficient to adequately and accurately quantify inpatient mortality risk. The addition of other common frailty factors that account for does not enhance the STTGMA tool's predictive capabilities.
老年创伤人群的虚弱与发病和死亡风险增加相关。老年和中年创伤分诊评分(STTGMA)是一种经过验证的死亡风险评分,它评估4个主要生理标准:年龄、合并症、生命体征和解剖损伤。本研究的目的是调查在STTGMA工具中增加额外的虚弱变量是否会改善中老年创伤人群的风险分层。
纳入2014年9月至2016年9月期间符合美国外科医师学会1至3级标准和/或在急诊科接受骨科或神经外科创伤会诊的1486例55岁及以上患者。计算STTGMA和STTGMA评分。额外的“虚弱变量”包括受伤前辅助设备使用情况(残疾)、独立行走状态(功能独立性)和白蛋白水平(营养)。使用受试者操作特征曲线下面积(AUROC)比较STTGMA和STTGMA模型预测住院死亡率的能力。
有23例高能量住院死亡(4.7%)和20例低能量住院死亡(2.0%)。使用STTGMA模型时,高能量和低能量队列的AUROC分别为0.926和0.896。高能量和低能量队列的STTGMA的AUROC分别为0.905和0.937。对于高能量和低能量队列,STTGMA和STTGMA在预测住院死亡率的能力上没有显著差异。
原始的STTGMA工具考虑了包括认知和一般健康状况在内的重要虚弱因素。这些变量与年龄和解剖损伤等其他主要生理变量相结合,似乎足以充分且准确地量化住院死亡率风险。添加其他常见的虚弱因素并不能增强STTGMA工具的预测能力。