Upper Gastrointestinal Surgery, Department of Molecular medicine and Surgery, Karolinska Institutet, Karolinska University Hospital, 17176, Stockholm, Sweden.
Cancer and Translational Medicine Research Unit, Medical Research Center, University of Oulu and Oulu University Hospital, 90014, Oulu, Finland.
Sci Rep. 2018 Jan 11;8(1):446. doi: 10.1038/s41598-017-18879-6.
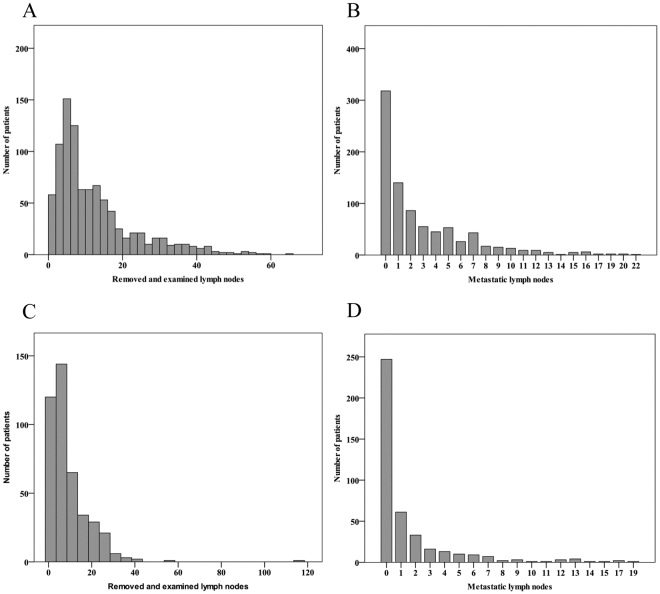
Differences in lymph node yield and tumour-involved resection margins comparing neoadjuvant therapy plus surgery with surgery alone for oesophageal cancer are unclear. Patients who underwent oesophageal cancer surgery in Sweden in 1987-2010 were included. Patients treated with neoadjuvant therapy were compared with those who underwent surgery alone. Outcomes were the number of examined lymph nodes (main outcome), number metastatic lymph nodes, and resection margin status. Rate ratios (RRs) and 95% CIs of lymph node yield were calculated by Poisson regression, and odds ratios (ORs) and 95% CIs of resection margin status by multivariable logistic regression, both adjusted for confounders. Among 1818 patients, 587 (32%) had received neoadjuvant therapy and 1231 (68%) had not. Lymph node yield was lower in the neoadjuvant therapy group (median 6 versus 8; adjusted RR 0.75, 0.73-0.78). Fewer metastatic nodes were identified following neoadjuvant therapy (median 0 versus 1; adjusted RR 0.76, 0.69-0.84). Neoadjuvant therapy associated to decreased risk of tumour-involved resection margins when adjusted for confounders except T-stage (OR 0.52, 0.38-0.70), but the association did not remain after adjustment for T-stage (OR 0.91, 0.64-1.29). Neoadjuvant therapy seems to decrease the lymph node yield and decrease the risk of tumour-involved resection margins by shrinking primary tumour.
新辅助治疗联合手术与单纯手术治疗食管癌的淋巴结检出量和肿瘤累及切缘的差异尚不清楚。纳入了 1987-2010 年在瑞典接受食管癌手术的患者。比较了接受新辅助治疗的患者和单纯手术的患者。结局为检查的淋巴结数量(主要结局)、转移淋巴结数量和切缘状态。采用泊松回归计算淋巴结检出量的率比(RR)及其 95%置信区间(CI),采用多变量逻辑回归计算切缘状态的比值比(OR)及其 95%CI,均调整了混杂因素。在 1818 例患者中,587 例(32%)接受了新辅助治疗,1231 例(68%)未接受。新辅助治疗组的淋巴结检出量较低(中位数 6 对 8;调整 RR 0.75,0.73-0.78)。新辅助治疗后,检出的转移淋巴结数量较少(中位数 0 对 1;调整 RR 0.76,0.69-0.84)。在调整了混杂因素(除 T 分期外)后,新辅助治疗与肿瘤累及切缘的风险降低相关(OR 0.52,0.38-0.70),但在调整 T 分期后,相关性不再存在(OR 0.91,0.64-1.29)。新辅助治疗似乎通过缩小原发肿瘤来降低淋巴结检出量和肿瘤累及切缘的风险。