Pediatric Endocrine Unit, Massachusetts General Hospital, Boston, MA.
Department of Pediatrics, Harvard Medical School, Boston, MA.
Diabetes Care. 2018 Mar;41(3):554-561. doi: 10.2337/dc17-1386. Epub 2018 Jan 11.
The rs7903146 T allele in transcription factor 7 like 2 () is strongly associated with type 2 diabetes (T2D), but the mechanisms for increased risk remain unclear. We evaluated the physiologic and hormonal effects of genotype before and after interventions that influence glucose physiology.
We genotyped rs7903146 in 608 individuals without diabetes and recorded biochemical data before and after ) one dose of glipizide (5 mg) on visit 1 and ) a 75-g oral glucose tolerance test (OGTT) performed after administration of metformin 500 mg twice daily over 2 days. Incretin levels were measured in 150 of the 608 participants.
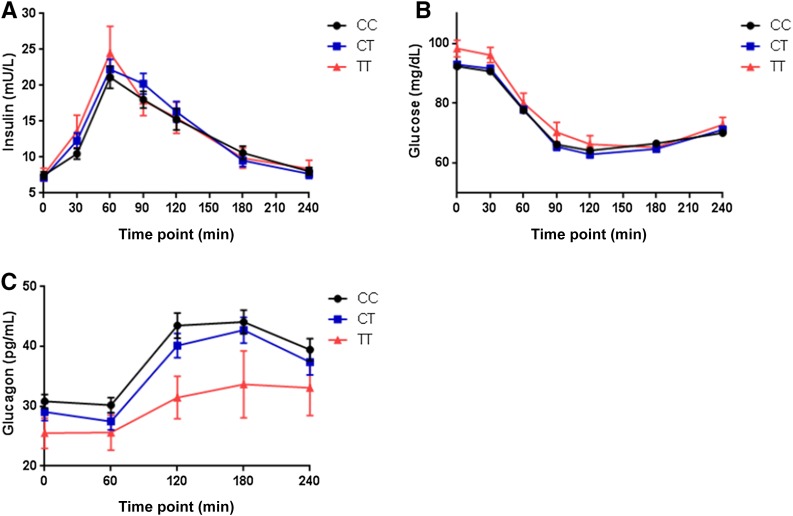
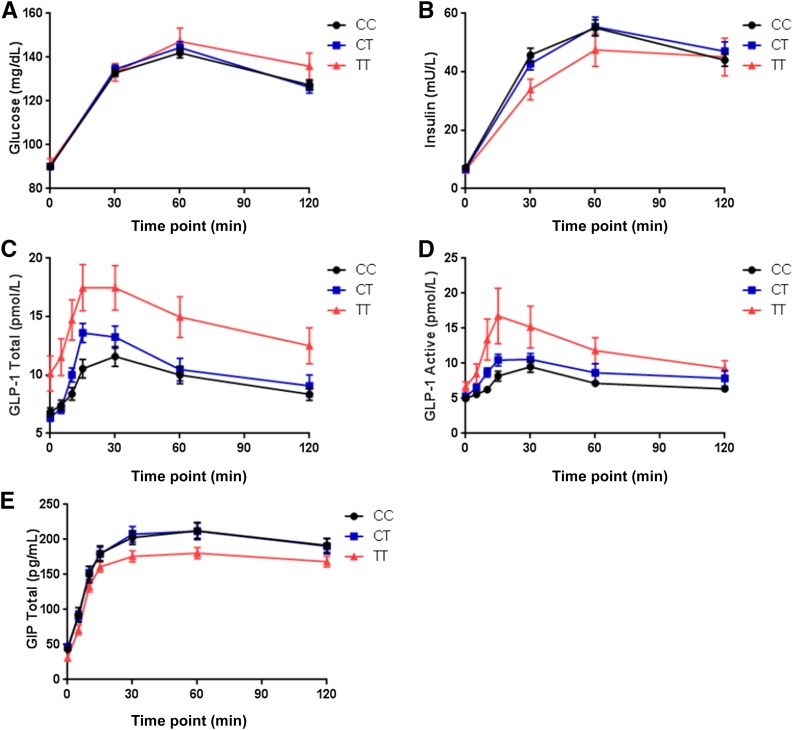
TT risk-allele homozygotes had 1.6 mg/dL higher baseline fasting glucose levels and 2.5 pg/mL lower glucagon levels per T allele than carriers of other genotypes at baseline. In a subset of participants, the T allele was associated with higher basal glucagon-like peptide 1 (GLP-1) levels at visit 1 (β = 1.52, = 0.02 and β = 0.96, = 0.002 for total and active GLP-1, respectively), and across all points of the OGTT after metformin administration. Regarding drug response, the T allele was associated with a shorter time (β = -7.00, = 0.03) and a steeper slope (β = 0.23, = 0.04) to trough glucose levels after glipizide administration, and lower visit 2 fasting glucose level adjusted for visit 1 fasting glucose level (β = -1.02, = 0.04) and a greater decline in glucose level between visits (β = -1.61, = 0.047) after metformin administration.
Our findings demonstrate that common variation at influences acute responses to both glipizide and metformin in people without diabetes and highlight altered incretin signaling as a potential mechanism by which variation increases T2D risk.
转录因子 7 样 2()基因中的 rs7903146T 等位基因与 2 型糖尿病(T2D)强烈相关,但增加风险的机制仍不清楚。我们评估了影响葡萄糖生理的干预措施前后基因型的生理和激素效应。
我们对 608 名无糖尿病个体进行了 rs7903146 基因分型,并在第 1 次就诊时记录了一次格列吡嗪(5mg)给药前后的生化数据,以及在二甲双胍 500mg 每日两次给药 2 天后进行 75g 口服葡萄糖耐量试验(OGTT)前后的生化数据。在 608 名参与者中的 150 名测量了肠降血糖素水平。
TT 风险等位基因纯合子在基线空腹血糖水平上比其他基因型携带者高 1.6mg/dL,在基础胰高血糖素水平上低 2.5pg/mL。在一部分参与者中,T 等位基因与第 1 次就诊时基础胰高血糖素样肽 1(GLP-1)水平升高相关(β=1.52,=0.02 和β=0.96,=0.002 分别用于总和活性 GLP-1),并且在二甲双胍给药后 OGTT 的所有点均升高。关于药物反应,T 等位基因与格列吡嗪给药后达到低谷血糖水平的时间(β=-7.00,=0.03)和斜率(β=0.23,=0.04)更短相关,并且在二甲双胍给药后,调整第 1 次就诊时的空腹血糖水平后,第 2 次就诊时的空腹血糖水平较低(β=-1.02,=0.04),两次就诊之间的血糖水平下降较大(β=-1.61,=0.047)。
我们的研究结果表明,在无糖尿病个体中,常见的 变异影响格列吡嗪和二甲双胍的急性反应,并强调了肠降血糖素信号的改变可能是 变异增加 T2D 风险的机制。