Cone Health, 1200 N. Elm Street, Greensboro, NC, 27401, USA.
Alamance Regional Cancer Center, Cone Health, 1240 Huffman Mill Road, Burlington, NC, 27215, USA.
Support Care Cancer. 2018 Jun;26(6):2031-2038. doi: 10.1007/s00520-017-4035-7. Epub 2018 Jan 19.
The decision to prescribe packed red blood cell (PRBC) transfusions in patients with chemotherapy-induced anemia (CIA) includes assessment of clinical features such as the patient's cancer type and treatment regimen, severity of anemia symptoms, and presence of comorbidities. We examined contemporary transfusion practices in patients with nonmyeloid cancer and CIA.
Key inclusion criteria were age ≥ 18 years with nonmyeloid cancer, receiving first/second-line myelosuppressive chemotherapy, baseline hemoglobin (Hb) ≤ 10.0 g/dL, and planned to receive ≥ 1 PRBC transfusions. Exclusion criteria were receipt of erythropoiesis-stimulating agents within 8 weeks of screening and/or chronic renal insufficiency. Data were collected from patients' medical records, laboratory values, and physician/provider questionnaires. Proportion of patients for each clinical consideration leading to a decision to prescribe a PRBC transfusion and 95% exact binomial confidence intervals were determined.
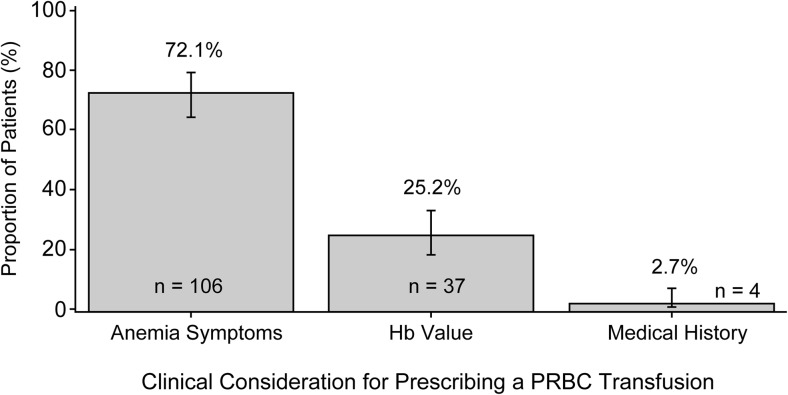
The study enrolled 154 patients at 18 sites in USA; 147 (95.5%) received a PRBC transfusion. Fatigue was the most common symptom affecting the decision to prescribe a PRBC transfusion (101 [69.2%] patients). Of the three reasons selected as primary considerations for prescribing a PRBC transfusion, anemia symptoms (106 [72.1%] patients) was the most frequently reported, followed by Hb value (37 [25.2%] patients) and medical history (4 [2.7%] patients).
In this study, the primary consideration for prescribing a PRBC transfusion was anemia symptoms in 72.1% of patients, with only 25.2% of patients prescribed a transfusion based exclusively on Hb value. Results indicate that clinical judgment and patient symptoms, not just Hb value, were used in decisions to prescribe PRBC transfusions.
在化疗引起的贫血(CIA)患者中决定是否开处浓缩红细胞(PRBC)输注包括评估患者的癌症类型和治疗方案、贫血症状的严重程度以及合并症等临床特征。我们研究了非髓性癌症伴 CIA 患者的当代输血实践。
主要纳入标准为年龄≥18 岁,患有非髓性癌症,接受一线/二线骨髓抑制化疗,基线血红蛋白(Hb)≤10.0g/dL,并计划接受≥1 次 PRBC 输注。排除标准为在筛选前 8 周内接受红细胞生成刺激剂治疗和/或慢性肾功能不全。数据从患者病历、实验室值和医生/提供者问卷中收集。确定了每个临床考虑因素导致决定开处 PRBC 输注的患者比例以及 95%确切二项式置信区间。
该研究在美国 18 个地点纳入了 154 例患者;147 例(95.5%)接受了 PRBC 输注。疲劳是影响决定开处 PRBC 输注的最常见症状(101 例[69.2%]患者)。在选择的三个输注主要考虑因素中,贫血症状(106 例[72.1%]患者)是最常报告的原因,其次是 Hb 值(37 例[25.2%]患者)和病史(4 例[2.7%]患者)。
在这项研究中,决定开处 PRBC 输注的主要考虑因素是 72.1%患者的贫血症状,只有 25.2%的患者仅根据 Hb 值开处输血。结果表明,在决定开处 PRBC 输注时,临床判断和患者症状而非仅仅 Hb 值被用于决策。