Masarone Daniele, Limongelli Giuseppe, Rubino Marta, Valente Fabio, Vastarella Rossella, Ammendola Ernesto, Gravino Rita, Verrengia Marina, Salerno Gemma, Pacileo Giuseppe
Cardiologia SUN-Heart Failure Unit, Department of Cardiothoracic Sciences, Second University of Naples, via L. Bianchi, Naples 80100, Italy.
J Cardiovasc Dev Dis. 2017 Feb 28;4(1):3. doi: 10.3390/jcdd4010003.
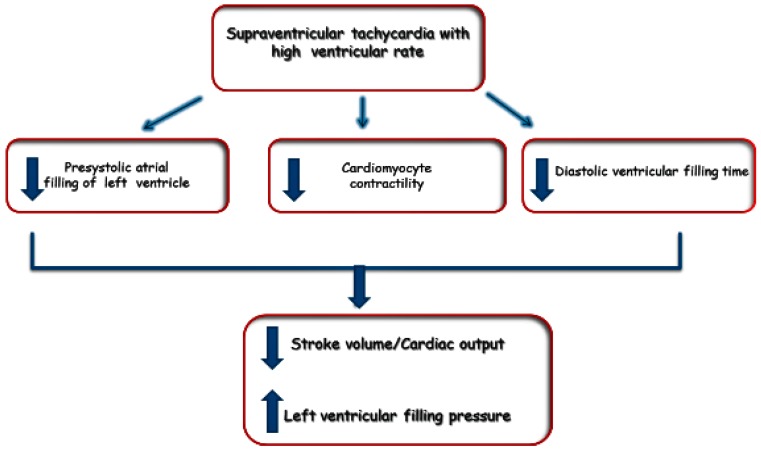
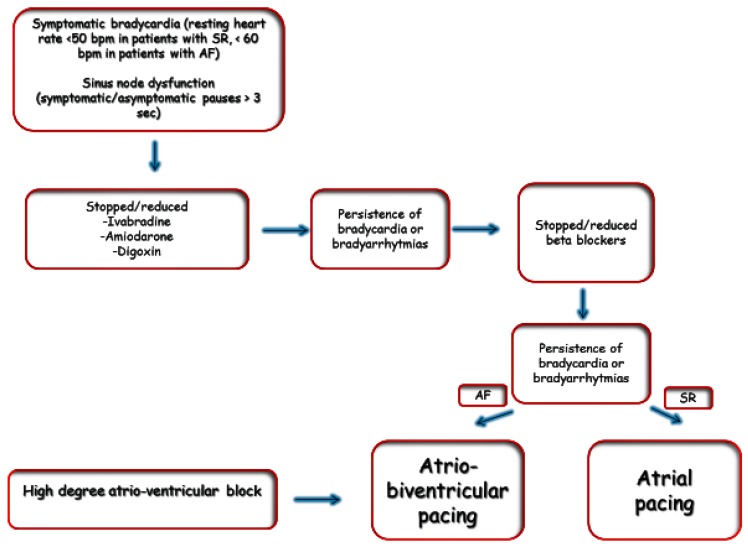
Heart failure patients are predisposed to develop arrhythmias. Supraventricular arrhythmias can exacerbate the heart failure symptoms by decreasing the effective cardiac output and their control require pharmacological, electrical, or catheter-based intervention. In the setting of atrial flutter or atrial fibrillation, anticoagulation becomes paramount to prevent systemic or cerebral embolism. Patients with heart failure are also prone to develop ventricular arrhythmias that can present a challenge to the managing clinician. The management strategy depends on the type of arrhythmia, the underlying structural heart disease, the severity of heart failure, and the range from optimization of heart failure therapy to catheter ablation. Patients with heart failure, irrespective of ejection fraction are at high risk for developing sudden cardiac death, however risk stratification is a clinical challenge and requires a multiparametric evaluation for identification of patients who should undergo implantation of a cardioverter defibrillator. Finally, patients with heart failure can also develop symptomatic bradycardia, caused by sinus node dysfunction or atrio-ventricular block. The treatment of bradycardia in these patients with pacing is usually straightforward but needs some specific issue.
心力衰竭患者易发生心律失常。室上性心律失常可通过降低有效心输出量而加重心力衰竭症状,控制此类心律失常需要药物、电或基于导管的干预措施。在心房扑动或心房颤动的情况下,抗凝对于预防全身性或脑栓塞至关重要。心力衰竭患者也容易发生室性心律失常,这对临床管理人员构成挑战。管理策略取决于心律失常的类型、潜在的结构性心脏病、心力衰竭的严重程度以及从优化心力衰竭治疗到导管消融的范围。无论射血分数如何,心力衰竭患者发生心源性猝死的风险都很高,然而风险分层是一项临床挑战,需要进行多参数评估以识别应接受植入式心脏复律除颤器的患者。最后,心力衰竭患者也可能出现由窦房结功能障碍或房室传导阻滞引起的症状性心动过缓。这些患者通过起搏治疗心动过缓通常较为直接,但需要注意一些特定问题。