Sage Michaël, Nadeau Mathieu, Forand-Choinière Claudia, Mousseau Julien, Vandamme Jonathan, Berger Claire, Tremblay-Roy Jean-Sébastien, Tissier Renaud, Micheau Philippe, Fortin-Pellerin Étienne
Department of Pediatrics and Department of Pharmacology and Physiology, Université de Sherbrooke, Sherbrooke, Québec, Canada.
Department of Mechanical Engineering, Université de Sherbrooke, Sherbrooke, Québec, Canada.
PLoS One. 2018 Jan 29;13(1):e0191885. doi: 10.1371/journal.pone.0191885. eCollection 2018.
Filling the lung with dense liquid perfluorocarbons during total liquid ventilation (TLV) might compress the myocardium, a plausible explanation for the instability occasionally reported with this technique. Our objective is to assess the impacts of TLV on the cardiovascular system, particularly left ventricular diastolic function, in an ovine model of neonatal respiratory distress syndrome.
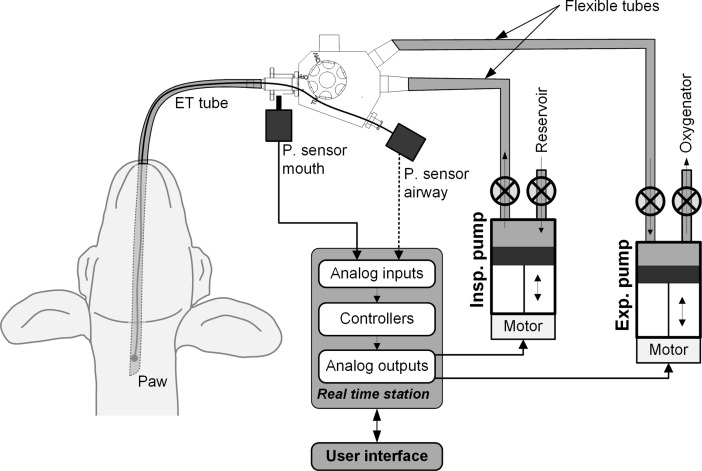
Eight newborns lambs, 3.0 ± 0.4 days (3.2 ± 0.3kg) were used in this crossover experimental study. Animals were intubated, anesthetized and paralyzed. Catheters were inserted in the femoral and pulmonary arteries. A high-fidelity pressure catheter was inserted into the left ventricle. Surfactant deficiency was induced by repeated lung lavages with normal saline. TLV was then conducted for 2 hours using a liquid ventilator prototype. Thoracic echocardiography and cardiac output assessment by thermodilution were performed before and during TLV.
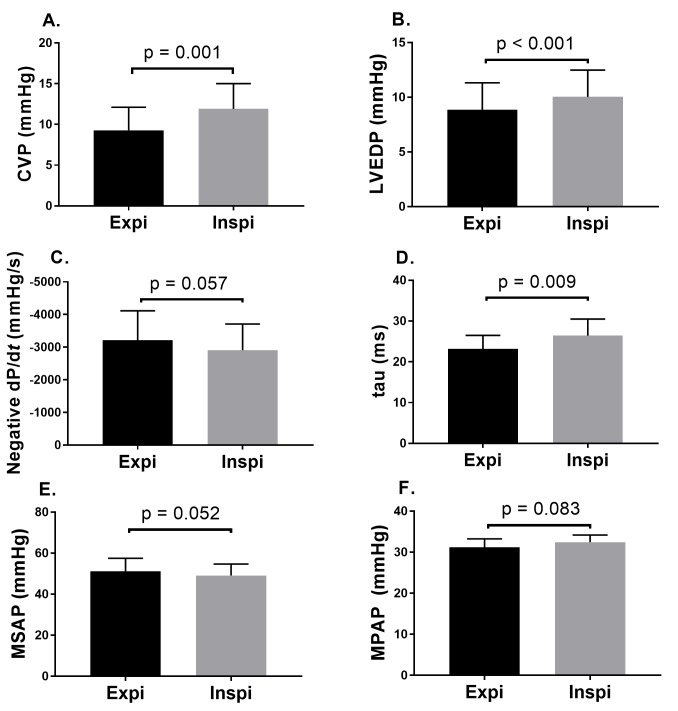
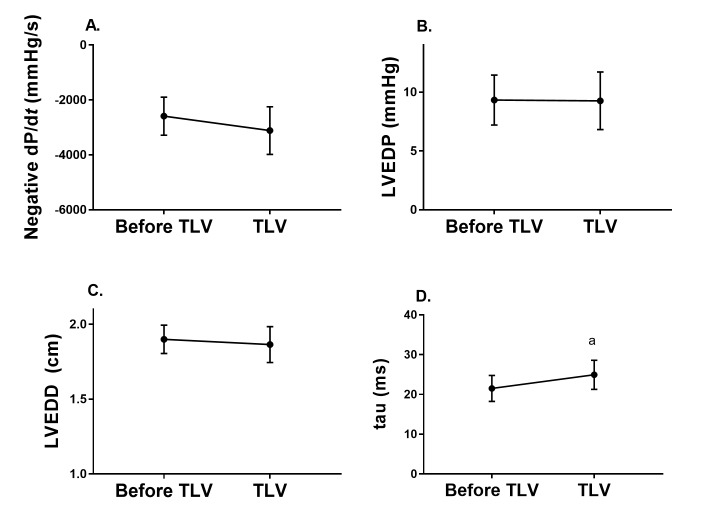
Left ventricular end diastolic pressure (LVEDP) (9.3 ± 2.1 vs. 9.2 ± 2.4mmHg, p = 0.89) and dimension (1.90 ± 0.09 vs. 1.86 ± 0.12cm, p = 0.72), negative dP/dt (-2589 ± 691 vs. -3115 ± 866mmHg/s, p = 0.50) and cardiac output (436 ± 28 vs. 481 ± 59ml/kg/min, p = 0.26) were not affected by TLV initiation. Left ventricular relaxation time constant (tau) slightly increased from 21.5 ± 3.3 to 24.9 ± 3.7ms (p = 0.03). Mean arterial systemic (48 ± 6 vs. 53 ± 7mmHg, p = 0.38) and pulmonary pressures (31.3 ± 2.5 vs. 30.4 ± 2.3mmHg, p = 0.61) were stable. As expected, the inspiratory phase of liquid cycling exhibited a small but significant effect on most variables (i.e. central venous pressure +2.6 ± 0.5mmHg, p = 0.001; LVEDP +1.18 ± 0.12mmHg, p<0.001).
TLV was well tolerated in our neonatal lamb model of severe respiratory distress syndrome and had limited impact on left ventricle diastolic function when compared to conventional mechanical ventilation.
在全液体通气(TLV)期间用高密度液体全氟碳化合物充盈肺脏可能会压迫心肌,这是该技术偶尔报告的不稳定性的一个合理的解释。我们的目的是在新生羊呼吸窘迫综合征的绵羊模型中评估TLV对心血管系统的影响,特别是左心室舒张功能。
在这项交叉实验研究中使用了8只新生羔羊,年龄为3.0±0.4天(体重3.2±0.3千克)。动物进行气管插管、麻醉和肌肉松弛。将导管插入股动脉和肺动脉。将一个高保真压力导管插入左心室。通过用生理盐水反复灌洗肺脏诱导表面活性剂缺乏。然后使用液体通气机原型进行2小时的TLV。在TLV之前和期间进行胸部超声心动图检查和通过热稀释法评估心输出量。
左心室舒张末期压力(LVEDP)(9.3±2.1对9.2±2.4mmHg,p = 0.89)和内径(1.90±0.09对1.86±0.12cm,p = 0.72)、负dP/dt(-2589±691对-3115±866mmHg/s,p = 0.50)和心输出量(436±28对481±59ml/kg/min,p = 0.26)不受TLV启动的影响。左心室舒张时间常数(tau)从21.5±3.3略微增加到24.9±3.7ms(p = 0.03)。平均动脉系统压力(48±6对53±7mmHg,p = 0.38)和肺动脉压力(31.3±2.5对30.4±2.3mmHg,p = 0.61)保持稳定。正如预期的那样,液体循环的吸气阶段对大多数变量有微小但显著的影响(即中心静脉压+2.6±0.5mmHg,p = 0.001;LVEDP +1.18±0.12mmHg,p<0.001)。
在我们的严重呼吸窘迫综合征新生羊模型中,TLV耐受性良好,与传统机械通气相比,对左心室舒张功能的影响有限。