Wang Lei, Liu Zhiqiang, Liu Xiaolong, Zeng Yongyi, Liu Jingfeng
The United Innovation of Mengchao Hepatobiliary Technology Key Laboratory of Fujian Province, Mengchao Hepatobiliary Hospital of Fujian Medical University The Liver Center of Fujian Province, Fujian Medical University Liver Disease Center, The First Affiliated Hospital of Fujian Medical University, Fuzhou, P. R. China.
Medicine (Baltimore). 2017 Dec;96(52):e9226. doi: 10.1097/MD.0000000000009226.
There has always been a controversy on the hepatectomy for huge hepatocellular carcinoma (HCC). Therefore, we aim to explore the hepatectomy efficacy of huge HCC and its risk factors.
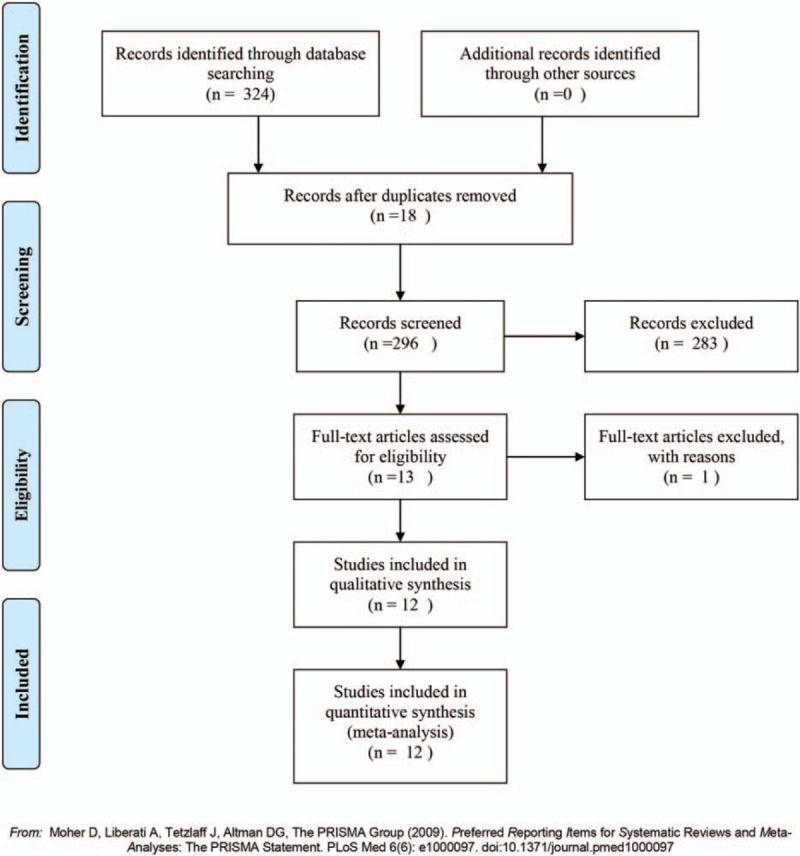
A systematic research was performed using PubMed, MedLine, Web of Knowledge, and Cochrane Library from their establishment to August 2017. The major endpoints were overall survival (OS) rate and recurrence-free survival (RFS) rate, and the secondary ones were the morbidity of complications and mortality of hepatectomy.
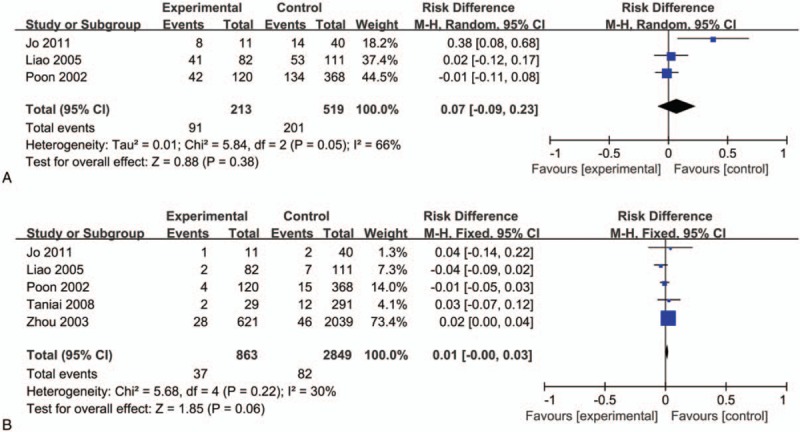
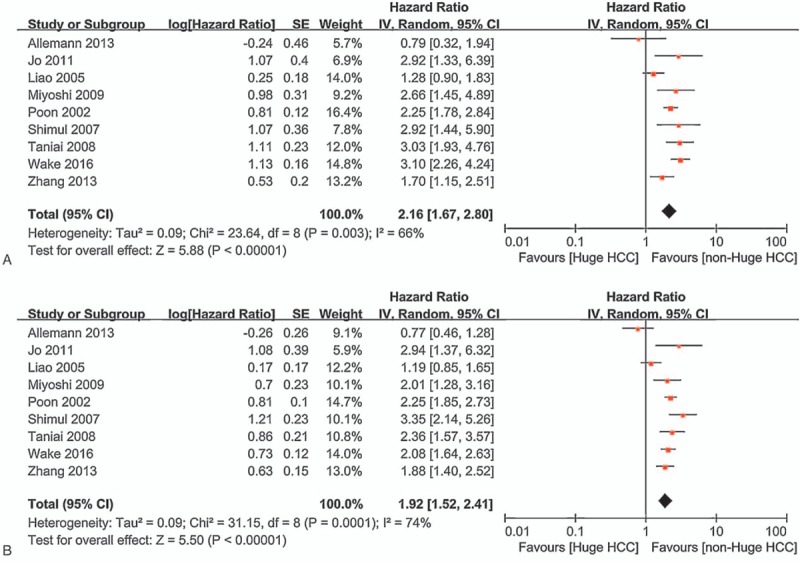
About 13 studies with a total of 7609 patients were included in this meta-analysis. The hepatectomy efficacy of huge HCC was inferior to non-huge HCC both in OS (hazard ratio [HR] = 2.18, 95% confidence interval [CI] = 1.90-2.50, P < .00001; I = 66%, P = .003) and RFS (HR = 1.97, 95% CI = 1.76-2.19, P < .00001; I = 74%, P = .0001). However, the risk difference[RD] of the 1-year, 3-year and 5-year OS tended to be acceptable (RD = -0.05, 95% CI = -0.11-0.00, P = .05; RD = -0.13, 95% CI = -0.21--0.05, P = .002; RD = -0.10, 95% CI = -0.19--0.01, P = .03; respectively). Moreover, there were also no significant differences between huge HCC and non-huge HCC in the morbidity of complication and mortality of hepatectomy (RD = 0.07, 95% CI = -0.09-0.23, P = .38; RD = -0.01, 95% CI = -0.00--0.03, P = .06; respectively). Related risk factors were measured to explore the differences, and the results showed that the level of alpha fetal protein (AFP) and the margin-positive rate were higher (standard mean difference [SMD] = 0.57, 95% CI = 0.26-0.88, P = .0003; odd radio[OR] = 32.52, 95% CI = 1.02-6.22, P = .04; respectively), the characteristic of huge HCC tended to be worse such as lower clinical or pathological stage, incomplete capsule and incorporate satellite metastases (OR = 2.91, 95% CI = 1.68-5.04, P = .001; OR = 3.99, 95% CI = 3.40-4.67, P < .00001; OR = 2.52, 95% CI = 1.66-3.83, P < .0001; respectively), and the rate of micorvascular invasion (MVI) including portal vein tumor thrombus (PVTT) were higher (OR = 3.36, 95% CI = 1.61-7.02, P = .001; OR = 2.75, 95% CI = 2.29-3.31, P < .00001; respectively) in the huge HCC.
The hepatectomy efficacy of huge HCC was inferior to non-huge HCC, but its survival benefits and feasibility were confirmed in this meta-analysis. In addition, higher level of AFP, positive margin, lower clinical or pathological stage, incomplete capsule, incorporate satellite metastasis and MVI were significantly correlated with poor OS.
巨大肝细胞癌(HCC)的肝切除术一直存在争议。因此,我们旨在探讨巨大HCC的肝切除疗效及其危险因素。
利用PubMed、MedLine、Web of Knowledge和Cochrane图书馆从建库至2017年8月进行系统研究。主要终点为总生存率(OS)和无复发生存率(RFS),次要终点为肝切除术后并发症发生率和死亡率。
本荟萃分析纳入了约13项研究,共7609例患者。巨大HCC的肝切除疗效在OS(风险比[HR]=2.18,95%置信区间[CI]=1.90 - 2.50,P<.00001;I=66%,P=.003)和RFS(HR=1.97,95%CI=1.76 - 2.19,P<.00001;I=74%,P=.0001)方面均低于非巨大HCC。然而,1年、3年和5年OS的风险差异[RD]趋于可接受(RD=-0.05,95%CI=-0.11 - 0.00,P=.05;RD=-0.13,95%CI=-0.21 - -0.05,P=.002;RD=-0.10,95%CI=-0.19 - -0.01,P=.03;分别)。此外,巨大HCC与非巨大HCC在肝切除术后并发症发生率和死亡率方面也无显著差异(RD=0.07,95%CI=-0.09 - 0.23,P=.38;RD=-0.01,95%CI=-0.00 - -0.03,P=.06;分别)。测量相关危险因素以探索差异,结果显示甲胎蛋白(AFP)水平和切缘阳性率较高(标准化均数差[SMD]=0.57,95%CI=0.26 - 0.88,P=.0003;比值比[OR]=32.52,95%CI=1.02 - 6.22,P=.04;分别),巨大HCC的特征往往更差,如临床或病理分期较低、包膜不完整和合并卫星转移(OR=2.91,95%CI=1.68 - 5.04,P=.001;OR=3.99,95%CI=3.40 - 4.67,P<.00001;OR=2.52,95%CI=1.66 - 3.83,P<.0001;分别),并且巨大HCC中微血管侵犯(MVI)包括门静脉癌栓(PVTT)的发生率较高(OR=3.36,95%CI=1.61 - 7.02,P=.001;OR=2.75,95%CI=2.29 - 3.31,P<.00001;分别)。
巨大HCC的肝切除疗效低于非巨大HCC,但本荟萃分析证实了其生存获益和可行性。此外,AFP水平较高、切缘阳性、临床或病理分期较低、包膜不完整、合并卫星转移和MVI与较差的OS显著相关。