Fischer Christin, Deininger Natalie, Wolf Gunter, Loeffler Ivonne
Department of Internal Medicine III, University Hospital Jena, Am Klinikum 1, D-07747 Jena, Germany.
Institute of Medical Genetics and Applied Genomics, University Tübingen, Calwerstraße 7, D-72076 Tübingen, Germany.
J Clin Med. 2018 Jan 30;7(2):15. doi: 10.3390/jcm7020015.
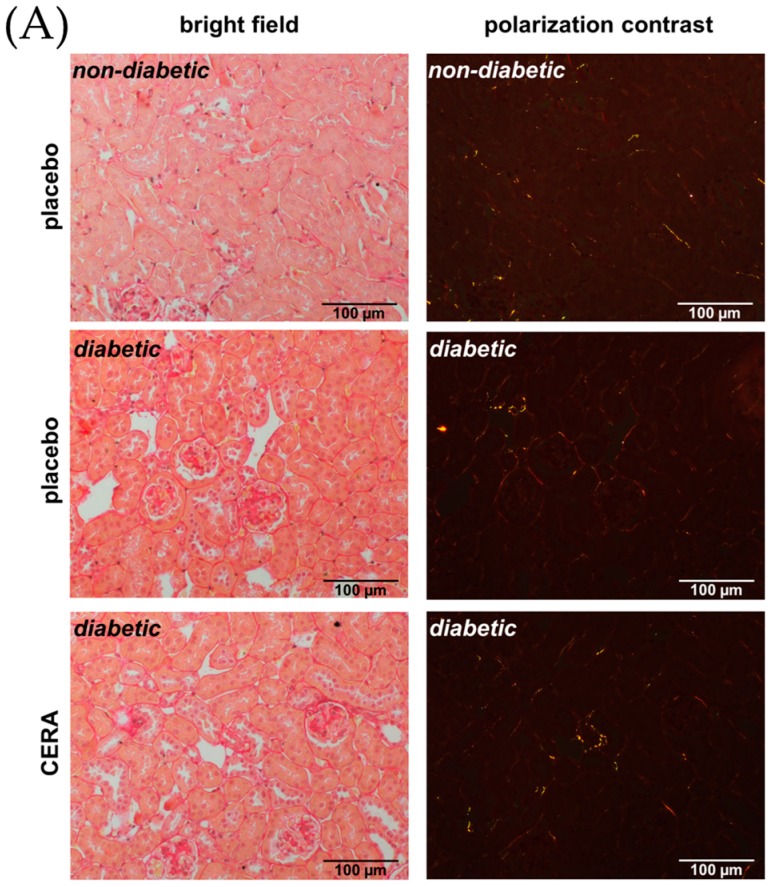
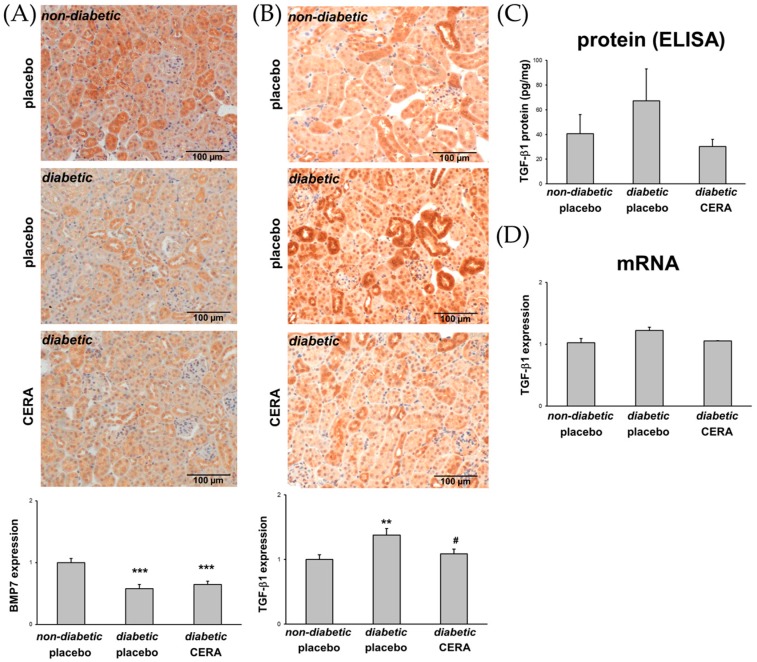
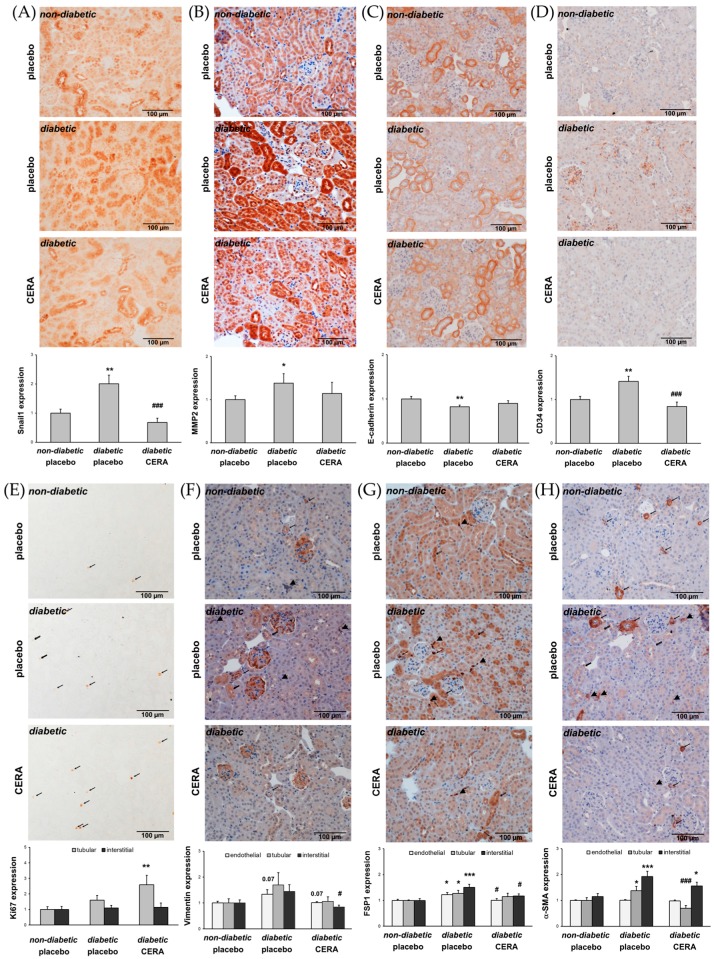
Tubulointerstitial fibrosis (TIF) is a pivotal pathophysiological process in patients with diabetic nephropathy (DN). Multiple profibrotic factors and cell types, including transforming growth factor beta 1 (TGF-β1) and interstitial myofibroblasts, respectively, are responsible for the accumulation of extracellular matrix in the kidney. Matrix-producing myofibroblasts can originate from different sources and different mechanisms are involved in the activation process of the myofibroblasts in the fibrotic kidney. In this study, 16-week-old / mice, a model for type 2 DN, were treated for two weeks with continuous erythropoietin receptor activator (CERA), a synthetic erythropoietin variant with possible non-hematopoietic, tissue-protective effects. Non-diabetic and diabetic mice treated with placebo were used as controls. The effects of CERA on tubulointerstitial fibrosis (TIF) as well as on the generation of the matrix-producing myofibroblasts were evaluated by morphological, immunohistochemical, and molecular biological methods. The placebo-treated diabetic mice showed significant signs of beginning renal TIF (shown by picrosirius red staining; increased connective tissue growth factor (CTGF), fibronectin and collagen I deposition; upregulated KIM1 expression) together with an increased number of interstitial myofibroblasts (shown by different mesenchymal markers), while kidneys from diabetic mice treated with CERA revealed less TIF and fewer myofibroblasts. The mechanisms, in which CERA acts as an anti-fibrotic agent/drug, seem to be multifaceted: first, CERA inhibits the generation of matrix-producing myofibroblasts and second, CERA increases the ability for tissue repair. Many of these CERA effects can be explained by the finding that CERA inhibits the renal expression of the cytokine TGF-β1.
肾小管间质纤维化(TIF)是糖尿病肾病(DN)患者关键的病理生理过程。多种促纤维化因子和细胞类型,分别包括转化生长因子β1(TGF-β1)和间质肌成纤维细胞,是肾脏细胞外基质积累的原因。产生基质的肌成纤维细胞可源自不同来源,且纤维化肾脏中肌成纤维细胞激活过程涉及不同机制。在本研究中,16周龄的2型糖尿病肾病模型小鼠连续两周接受促红细胞生成素受体激活剂(CERA)治疗,CERA是一种具有可能的非造血、组织保护作用的合成促红细胞生成素变体。用安慰剂治疗的非糖尿病和糖尿病小鼠作为对照。通过形态学、免疫组织化学和分子生物学方法评估CERA对肾小管间质纤维化(TIF)以及对产生基质的肌成纤维细胞生成的影响。用安慰剂治疗的糖尿病小鼠显示出肾脏TIF开始的显著迹象(用天狼星红染色显示;结缔组织生长因子(CTGF)、纤连蛋白和I型胶原沉积增加;KIM1表达上调),同时间质肌成纤维细胞数量增加(用不同间充质标志物显示),而用CERA治疗的糖尿病小鼠的肾脏显示出较少的TIF和较少的肌成纤维细胞。CERA作为抗纤维化药物发挥作用的机制似乎是多方面的:首先,CERA抑制产生基质的肌成纤维细胞的生成;其次,CERA增强组织修复能力。CERA的许多这些作用可以通过CERA抑制细胞因子TGF-β1在肾脏中的表达这一发现来解释。