Ball Benjamin Z, Pelargos Panayiotis E, Christie Catherine, Golshani Kiarash
Department of Neurological Surgery, University of California Irvine, Orange, California, USA.
Surg Neurol Int. 2018 Jan 16;9:7. doi: 10.4103/sni.sni_190_17. eCollection 2018.
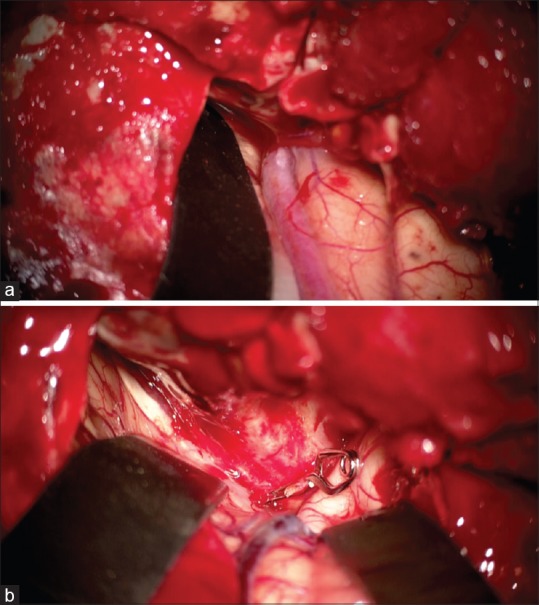
Direct, Type A, cavernous-carotid fistulas (CCFs) are predominantly caused by head trauma, especially when basilar skull fractures are present. Transarterial endovascular treatment of direct CCFs is the preferred method of treatment. Bilateral CCFs are estimated to be present in 1-2% of the cases. The treatment of bilateral CCFs is difficult often requiring a combination of endovascular and open surgical approaches.
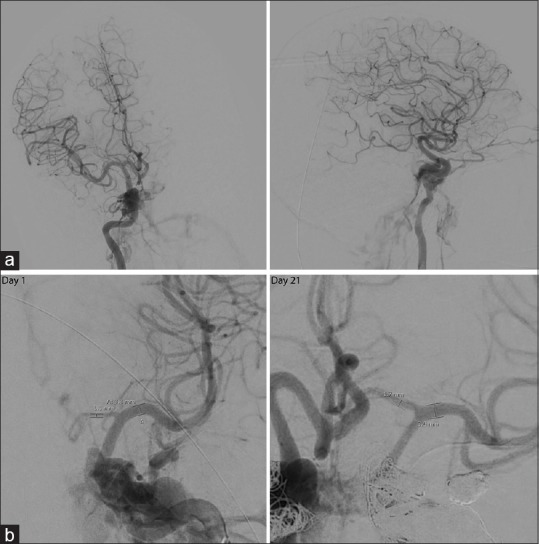
We present a case of traumatic bilateral CCFs presenting with vasospasm of the anterior circulation seen on the initial angiogram on day 1 and our treatment paradigm.
This case illustrates the challenges in managing bilateral CCFs as well as the changes in collateral circulation because of cerebral vasospasm which affected our treatment paradigm.
直接型 A 型海绵窦 - 颈动脉瘘(CCF)主要由头部外伤引起,尤其是存在颅底骨折时。经动脉血管内治疗直接型 CCF 是首选的治疗方法。据估计,双侧 CCF 在 1% - 2%的病例中出现。双侧 CCF 的治疗困难,通常需要血管内和开放手术方法相结合。
我们报告一例创伤性双侧 CCF 病例,在第 1 天的初始血管造影中可见前循环血管痉挛,以及我们的治疗模式。
本病例说明了双侧 CCF 管理中的挑战,以及由于脑血管痉挛导致的侧支循环变化,这影响了我们的治疗模式。