Kooiman Judith, de Vries Jean-Paul P M, Van der Heyden Jan, Sijpkens Yvo W J, van Dijkman Paul R M, Wever Jan J, van Overhagen Hans, Vahl Antonie C, Aarts Nico, Verberk-Jonkers Iris J A M, Brulez Harald F H, Hamming Jaap F, van der Molen Aart J, Cannegieter Suzanne C, Putter Hein, van den Hout Wilbert B, Kilicsoy Inci, Rabelink Ton J, Huisman Menno V
Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, the Netherlands.
Department of Nephrology, Leiden University Medical Center, Leiden, The Netherlands.
PLoS One. 2018 Feb 8;13(2):e0189372. doi: 10.1371/journal.pone.0189372. eCollection 2018.
Guidelines advise periprocedural saline hydration for prevention of contrast induced-acute kidney injury (CI-AKI). We analysed whether 1-hour sodium bicarbonate hydration administered solely prior to intra-arterial contrast exposure is non-inferior to standard periprocedural saline hydration in chronic kidney disease (CKD) patients undergoing elective cardiovascular diagnostic or interventional contrast procedures.
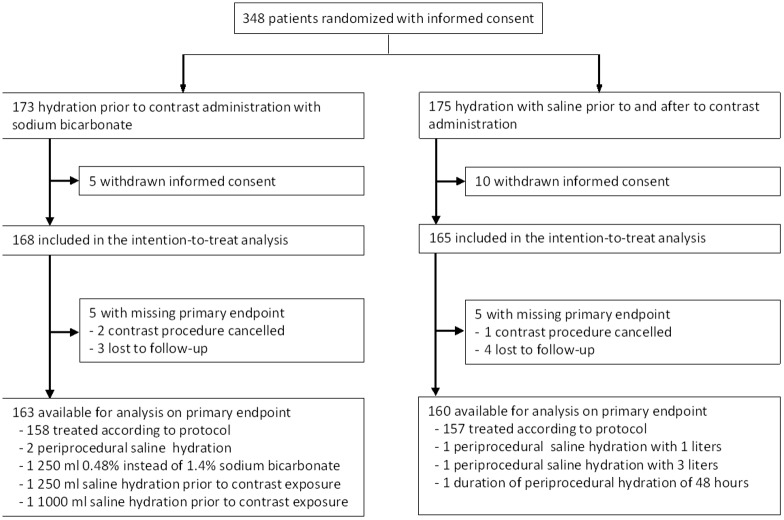
We performed an open-label multicentre non-inferiority trial between 2011-2014. Patients were randomized to 1 hour pre-procedure sodium bicarbonate hydration (250 ml 1.4%, N = 168) or 4-12 hours saline hydration (1000 ml 0.9%, N = 165) prior to and following contrast administration (2000 ml of saline total). Primary outcome was the relative serum creatinine increase (%) 48-96 hours post contrast exposure. Secondary outcomes were: incidence of CI-AKI (serum creatinine increase>25% or >44μmol/L), recovery of renal function, the need for dialysis, and hospital costs within two months follow-up.
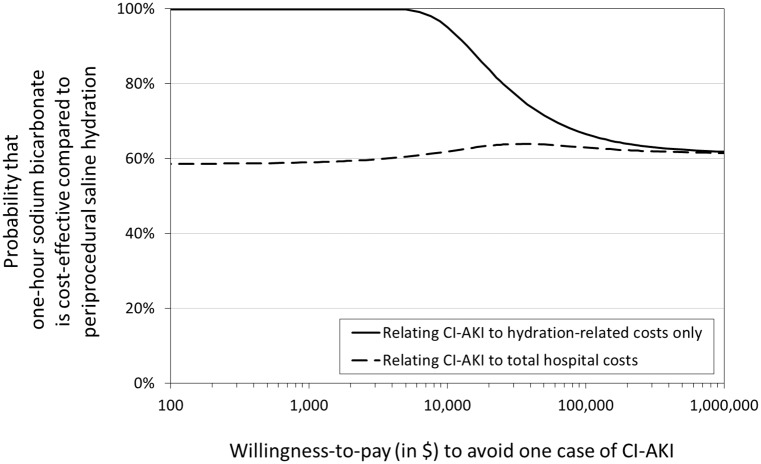
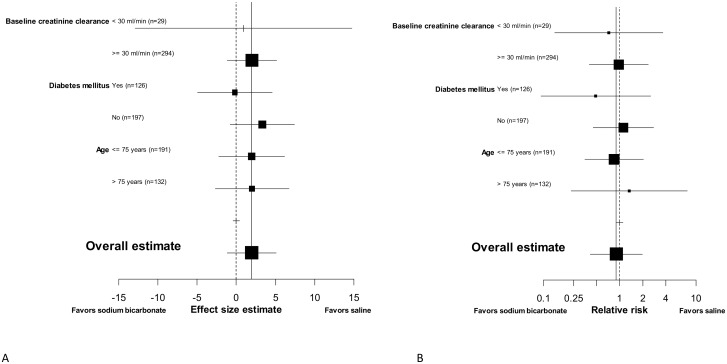
Mean relative creatinine increase was 3.1% (95%CI 0.9 to 5.2%) in the bicarbonate and 1.1% (95%CI -1.2 to 3.5%) in the saline arm, mean difference 1.9% (95%CI -1.2 to 5.1%, p-non-inferiority <0.001). CI-AKI occurred in 11 (6.7%) patients randomized to sodium bicarbonate and 12 (7.5%) to saline (p = 0.79). Renal function did not fully recover in 40.0% and 44.4% of CI-AKI patients, respectively (p = 0.84). No patient required dialysis. Mean costs for preventive hydration and clinical preparation for the contrast procedure were $1158 for sodium bicarbonate vs. $1561 for saline (p < 0.001).
Short hydration with sodium bicarbonate prior to elective cardiovascular diagnostic or therapeutic contrast procedures is non-inferior to standard periprocedural saline hydration in CKD patients with respect to renal safety and results in considerable healthcare savings.
Netherlands Trial Register (http://www.trialregister.nl/trialreg/index.asp), Nr NTR2699.
指南建议围手术期进行生理盐水水化以预防造影剂诱导的急性肾损伤(CI-AKI)。我们分析了在接受择期心血管诊断或介入造影检查的慢性肾脏病(CKD)患者中,仅在动脉内造影剂暴露前给予1小时碳酸氢钠水化是否不劣于标准围手术期生理盐水水化。
我们在2011年至2014年期间进行了一项开放标签的多中心非劣效性试验。患者被随机分为造影剂给药前1小时给予碳酸氢钠水化组(250ml 1.4%,N = 168)或造影剂给药前后给予4至12小时生理盐水水化组(1000ml 0.9%,N = 165)(共2000ml生理盐水)。主要结局是造影剂暴露后48至96小时血清肌酐相对升高百分比(%)。次要结局包括:CI-AKI的发生率(血清肌酐升高>25%或>44μmol/L)、肾功能恢复情况、透析需求以及随访两个月内的住院费用。
碳酸氢钠组血清肌酐平均相对升高3.1%(95%CI 0.9至5.2%),生理盐水组为1.1%(95%CI -1.2至3.5%),平均差异为1.9%(95%CI -1.2至5.1%,非劣效性p<0.001)。随机接受碳酸氢钠治疗的患者中有11例(6.7%)发生CI-AKI,接受生理盐水治疗的患者中有