Institute of Industrial Science, The University of Tokyo, 4-6-1 Komaba, Meguro-ku, Tokyo, 153-8505, Japan.
Department of Mathematical Informatics, The University of Tokyo, Tokyo, Japan.
Sci Rep. 2018 Feb 8;8(1):2673. doi: 10.1038/s41598-018-20788-1.
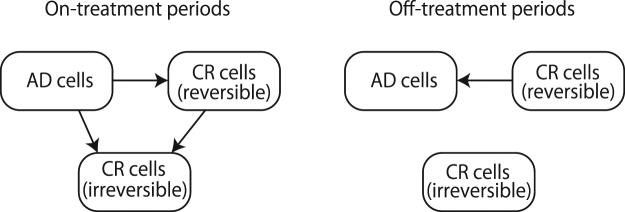
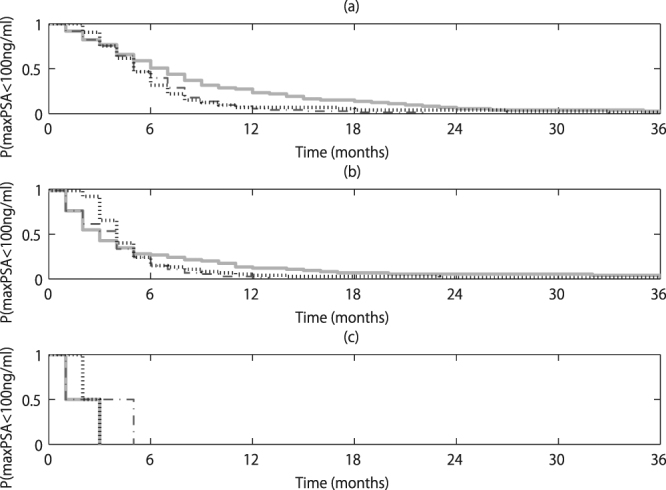
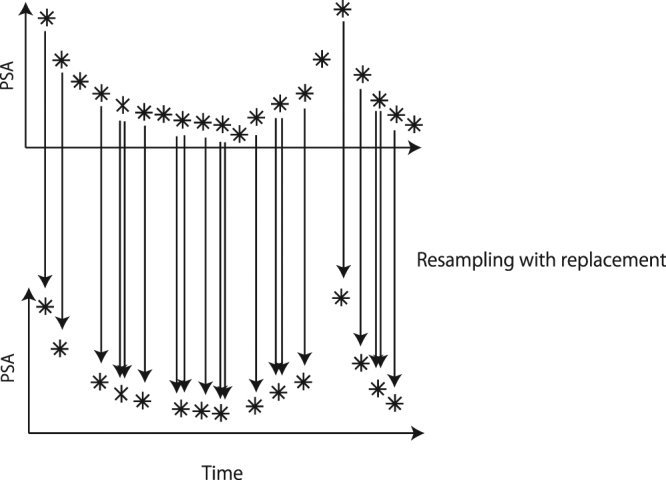
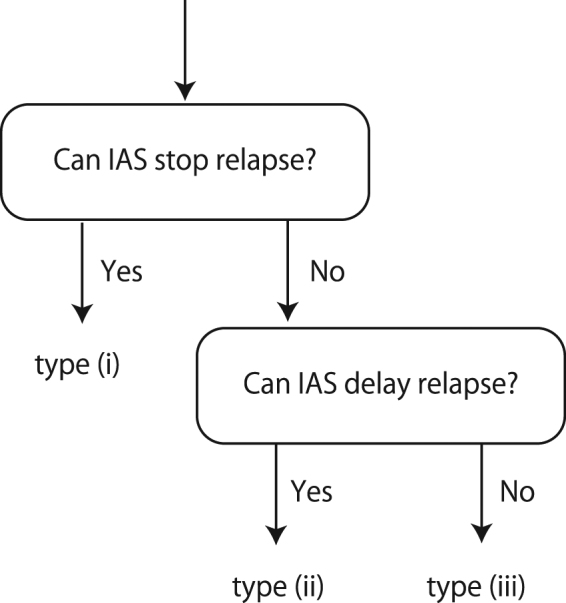
Using a dataset of 150 patients treated with intermittent androgen suppression (IAS) through a fixed treatment schedule, we retrospectively designed a personalized treatment schedule mathematically for each patient. We estimated 100 sets of parameter values for each patient by randomly resampling each patient's time points to take into account the uncertainty for observations of prostate specific antigen (PSA). Then, we identified 3 types and classified patients accordingly: in type (i), the relapse, namely the divergence of PSA, can be prevented by IAS; in type (ii), the relapse can be delayed by IAS later than by continuous androgen suppression (CAS); in type (iii) IAS was not beneficial and therefore CAS would have been more appropriate in the long run. Moreover, we obtained a treatment schedule of hormone therapy by minimizing the PSA of 3 years later in the worst case scenario among the 100 parameter sets by searching exhaustively all over the possible treatment schedules. If the most frequent type among 100 sets was type (i), the maximal PSA tended to be kept less than 100 ng/ml longer in IAS than in CAS, while there was no statistical difference for the other cases. Thus, mathematically personalized IAS should be studied prospectively.
我们使用了一组 150 名接受间歇性雄激素抑制(IAS)治疗的患者数据集,通过固定治疗方案,我们为每位患者数学上设计了个性化的治疗方案。我们通过随机重新采样每位患者的时间点,考虑到前列腺特异性抗原(PSA)观察的不确定性,为每位患者估计了 100 组参数值。然后,我们确定了 3 种类型,并相应地对患者进行了分类:在类型(i)中,IAS 可以预防复发,即 PSA 的离散;在类型(ii)中,IAS 可以比连续雄激素抑制(CAS)更延迟复发;在类型(iii)中,IAS 没有益处,因此从长远来看,CAS 会更合适。此外,我们通过在所有可能的治疗方案中进行穷尽搜索,找到了在 100 组参数中通过使 3 年后 PSA 最差情况最小化的激素治疗方案。如果 100 组中最常见的类型是类型(i),那么 IAS 中 PSA 保持在 100ng/ml 以下的时间将长于 CAS,而其他情况则没有统计学差异。因此,IAS 的个体化治疗应该进行前瞻性研究。