Croker Richard, Walker Alex J, Bacon Seb, Curtis Helen J, French Lisa, Goldacre Ben
Centre for Evidence Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
BMJ Open. 2018 Feb 8;8(2):e019643. doi: 10.1136/bmjopen-2017-019643.
Minimising prescription costs while maintaining quality is a core element of delivering high-value healthcare. There are various strategies to achieve savings, but almost no research to date on determining the most effective approach. We describe a new method of identifying potential savings due to large national variations in drug cost, including variation in generic drug cost, and compare these with potential savings from an established method (generic prescribing).
We used English National Health Service (NHS) Digital prescribing data, from October 2015 to September 2016. Potential cost savings were calculated by determining the price per unit (eg, pill, millilitre) for each drug and dose within each general practice. This was compared against the same cost for the practice at the lowest cost decile to determine achievable savings. We compared these price-per-unit savings to the savings possible from generic switching and determined the chemicals with the highest savings nationally. A senior pharmacist manually assessed whether a random sample of savings were practically achievable.
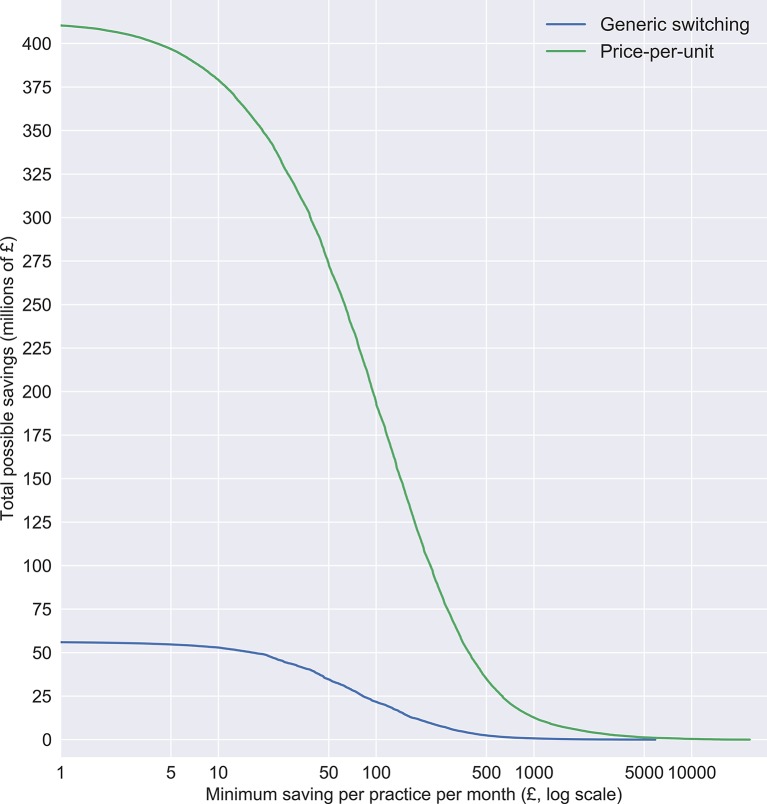
We identified a theoretical maximum of £410 million of savings over 12 months. £273 million of these savings were for individual prescribing changes worth over £50 per practice per month (mean annual saving £33 433 per practice); this compares favourably with generic switching, where only £35 million of achievable savings were identified. The biggest savings nationally were on glucose blood testing reagents (£12 million), fluticasone propionate (£9 million) and venlafaxine (£8 million). Approximately half of all savings were deemed practically achievable.
We have developed a new method to identify and enable large potential cost savings within NHS community prescribing. Given the current pressures on the NHS, it is vital that these potential savings are realised. Our tool enabling doctors to achieve these savings is now launched in pilot form at OpenPrescribing.net. However, savings could potentially be achieved more simply through national policy change.
在保持医疗质量的同时尽量降低处方成本是提供高价值医疗服务的核心要素。实现成本节约有多种策略,但迄今为止几乎没有关于确定最有效方法的研究。我们描述了一种新方法,用于识别因全国药品成本存在巨大差异(包括仿制药成本差异)而产生的潜在节约,并将这些节约与既定方法(开具仿制药)带来的潜在节约进行比较。
我们使用了英国国家医疗服务体系(NHS)数字化处方数据,时间跨度为2015年10月至2016年9月。通过确定每个全科诊所内每种药物和剂量的单位价格(例如,每片、每毫升)来计算潜在成本节约。将其与处于成本最低十分位数的诊所的相同成本进行比较,以确定可实现的节约。我们将这些单位价格节约与通过改用仿制药可能实现的节约进行比较,并确定全国节约最多的化学药品。一名资深药剂师手动评估了随机抽取的节约案例在实际中是否可行。
我们确定在12个月内理论上最多可节约4.1亿英镑。其中2.73亿英镑的节约来自于每个诊所每月价值超过50英镑的个人处方变更(每个诊所平均每年节约33433英镑);这与改用仿制药相比更具优势,改用仿制药仅确定了3500万英镑的可实现节约。全国节约最多的是血糖检测试剂(1200万英镑)、丙酸氟替卡松(900万英镑)和文拉法辛(800万英镑)。所有节约中约有一半被认为在实际中可行。
我们开发了一种新方法,用于识别并实现NHS社区处方中的巨大潜在成本节约。鉴于NHS目前面临的压力,实现这些潜在节约至关重要。我们使医生能够实现这些节约的工具现已以试点形式在OpenPrescribing.net上推出。然而,通过国家政策变革可能更简单地实现节约。