Department of Radiation Oncology, Mayo Clinic, Rochester, Minnesota.
Department of Radiation Oncology, Keck School of Medicine of USC, Los Angeles, California.
Cancer Med. 2018 Mar;7(3):757-764. doi: 10.1002/cam4.1352. Epub 2018 Feb 14.
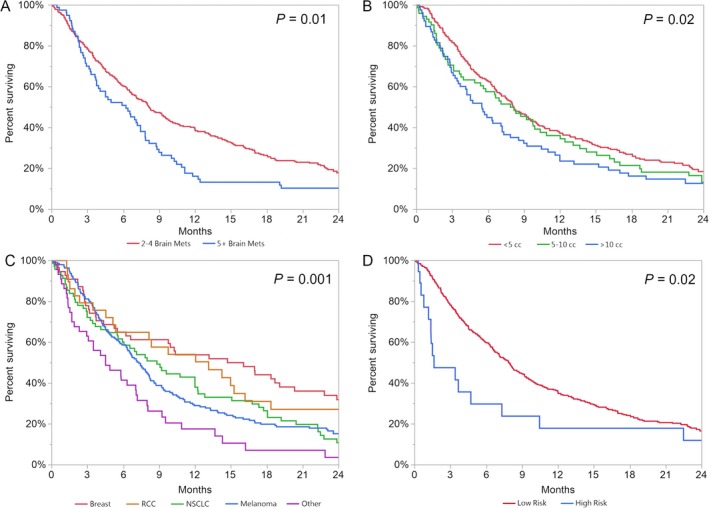
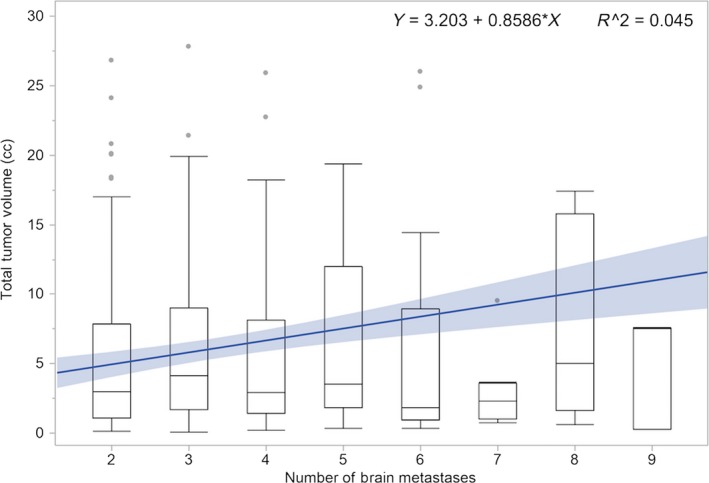
Stereotactic Radiosurgery (SRS) is considered standard of care for patients with 1-3 brain metastases (BM). Recent observational studies have shown equivalent OS in patients with 5+ BM compared to those with 2-4, suggesting SRS alone may be appropriate in these patients. We aim to review outcomes of patients treated with SRS with 2-4 versus 5+ BM. This analysis included consecutive patients from 1994 to 2015 treated with SRS. Of 1017 patients, we excluded patients with a single BM and patients without adequate survival data, resulting in 391 patients. All risk factors were entered into univariate analysis using Cox proportional hazards model, and significant factors were entered into multivariate analysis (MVA). We additionally analyzed outcomes after excluding patients with prior surgery or whole-brain radiotherapy (WBRT). Median follow-up was 7.1 months. Median KPS was 90, mean age was 59, and most common histologies were melanoma and lung. Median tumor volume was 3.41 cc. Patients with 2-4 BM had a median OS of 8.1 months compared to 6.2 months for those with 5+ BM (P = 0.0136). On MVA, tumor volume, KPS, and histology remained significant for OS, whereas lesion number did not. Similar results were found when excluding patients with prior surgery or WBRT. Rather than lesion number, the strongest prognostic factors for patients undergoing SRS were tumor volume >10 cc, KPS, and histology. BM number may therefore not be the most important criterion for candidacy for SRS. Patients with 5 or more BM should be considered for SRS.
立体定向放射外科(SRS)被认为是 1-3 个脑转移瘤(BM)患者的标准治疗方法。最近的观察性研究表明,5 个以上 BM 的患者与 2-4 个 BM 的患者的总生存期(OS)相当,这表明 SRS 单独治疗这些患者可能是合适的。我们旨在回顾 SRS 治疗 2-4 个与 5 个以上 BM 的患者的结果。该分析包括 1994 年至 2015 年期间连续接受 SRS 治疗的患者。在 1017 名患者中,我们排除了单个 BM 患者和无足够生存数据的患者,最终纳入 391 名患者。使用 Cox 比例风险模型对所有危险因素进行单因素分析,将有意义的因素纳入多因素分析(MVA)。我们还分析了排除既往手术或全脑放疗(WBRT)患者后的结果。中位随访时间为 7.1 个月。中位 KPS 为 90,平均年龄为 59 岁,最常见的组织学类型是黑色素瘤和肺癌。中位肿瘤体积为 3.41cc。2-4 个 BM 的患者中位 OS 为 8.1 个月,5 个以上 BM 的患者中位 OS 为 6.2 个月(P=0.0136)。在 MVA 中,肿瘤体积、KPS 和组织学对 OS 仍然具有显著意义,而病变数量则没有。当排除既往手术或 WBRT 的患者时,也得到了类似的结果。对于接受 SRS 的患者,肿瘤体积>10cc、KPS 和组织学是最强的预后因素,而病变数量并不是最重要的 SRS 候选标准。因此,应考虑 5 个或更多 BM 的患者进行 SRS。