Department of Surgery, Breast Oncology, NHO Osaka National Hospital, Osaka, Japan.
Department of Surgery (Breast Surgery), Kyoto University Graduate School of Medicine, 54 Kawahara-cho, Shogoin, Sakyo-ku, Kyoto, 606-8507, Japan.
Breast Cancer. 2018 Jul;25(4):407-415. doi: 10.1007/s12282-018-0839-7. Epub 2018 Feb 14.
Dual blockade of HER2 promises increased pathological complete response (pCR) rate compared with single blockade in the presence of chemotherapy for HER2-positive (+) primary breast cancer. Many questions remain regarding optimal duration of treatment and combination impact of endocrine therapy for luminal HER2 disease.
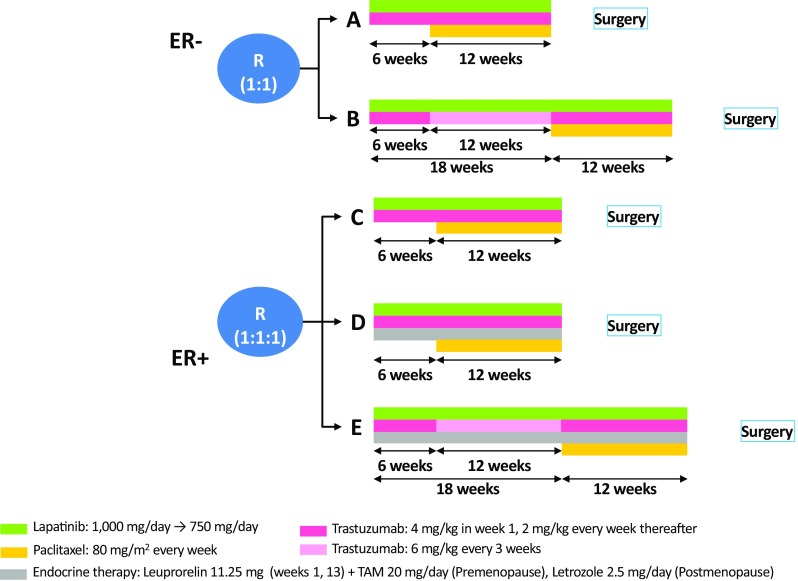
We designed a randomised phase II, five-arm study to evaluate the efficacy and safety of lapatinib and trastuzumab (6 weeks) followed by lapatinib and trastuzumab plus weekly paclitaxel (12 weeks) with/without prolongation of anti-HER2 therapy prior to chemotherapy (18 vs. 6 weeks), and with/without endocrine therapy in patients with HER2+ and/or oestrogen receptor (ER)+ disease. The primary endpoint was comprehensive pCR (CpCR) rate. Among the secondary endpoints, pCR (yT0-isyN0) rate, safety, and clinical response were evaluated.
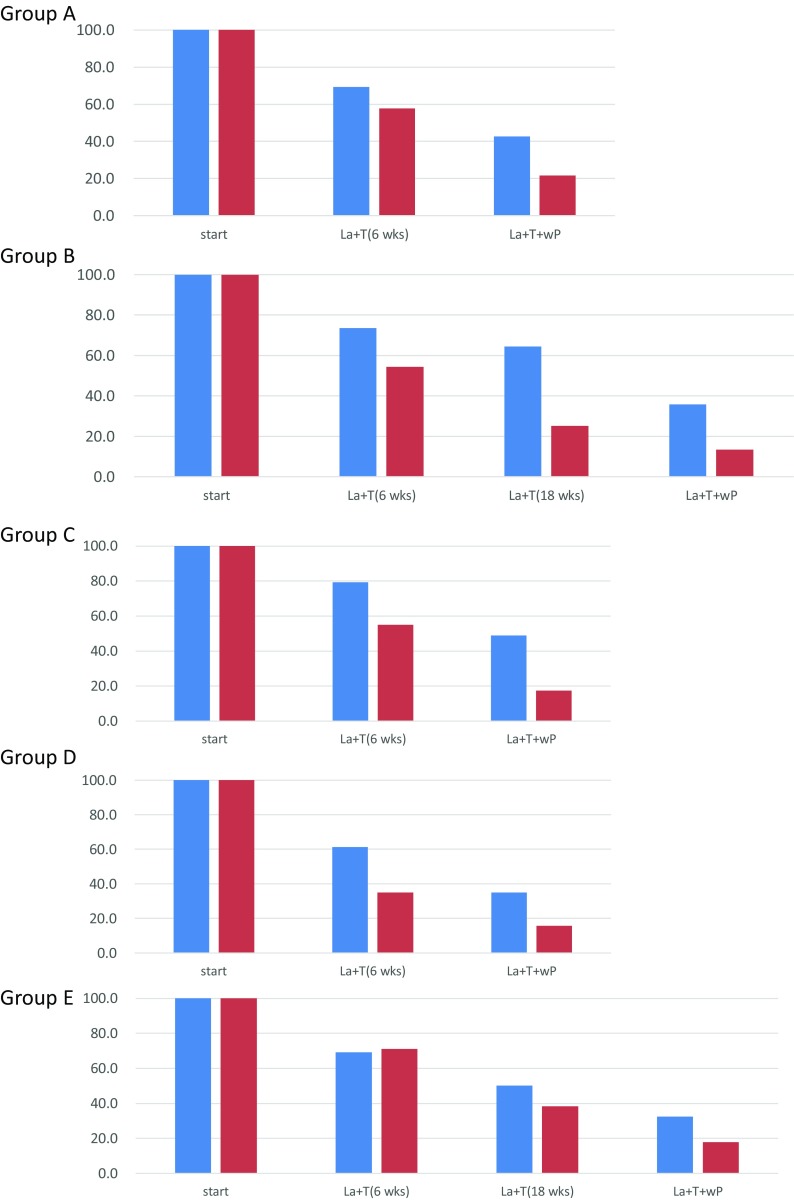
In total, 215 patients were enrolled; 212 were included in the full analysis set (median age 53.0 years; tumour size = T2, 65%; and tumour spread = N0, 55%). CpCR was achieved in 101 (47.9%) patients and was significantly higher in ER- patients than in ER+ patients (ER- 63.0%, ER+ 36.1%; P = 0.0034). pCR with pN0 was achieved in 42.2% of patients (ER- 57.6%, ER+ 30.3%). No significant difference was observed in pCR rate between prolonged exposure groups and standard groups. Better clinical response outcomes were obtained in the prolongation phase of the anti-HER2 therapy. No surplus was detected in pCR rate by adding endocrine treatment. No major safety concern was recognised by prolonging the anti-HER2 treatment or adding endocrine therapy.
This study confirmed the therapeutic impact of lapatinib, trastuzumab, and paclitaxel therapy for each ER- and ER+ subgroup of HER2+ patients. Development of further strategies and tools is required, particularly for luminal HER2 disease.
在存在化疗的情况下,HER2 阳性(+)原发性乳腺癌的双阻断比单阻断更能提高病理性完全缓解(pCR)率。对于 luminal HER2 疾病的最佳治疗持续时间和内分泌治疗的联合影响,仍存在许多问题。
我们设计了一项随机的 II 期、五臂研究,以评估 lapatinib 和曲妥珠单抗(6 周)继以 lapatinib 和曲妥珠单抗加每周紫杉醇(12 周)的疗效和安全性,同时考虑在化疗前延长抗 HER2 治疗(18 周对比 6 周),以及在 HER2+和/或雌激素受体(ER)+疾病患者中联合和/不联合内分泌治疗。主要终点是综合 pCR(CpCR)率。次要终点包括 pCR(yT0-isyN0)率、安全性和临床反应。
共纳入 215 例患者,212 例患者纳入全分析集(中位年龄 53.0 岁;肿瘤大小=T2,65%;肿瘤扩散=N0,55%)。101 例(47.9%)患者达到 CpCR,ER-患者明显高于 ER+患者(ER-63.0%,ER+36.1%;P=0.0034)。pN0 患者 pCR 率为 42.2%(ER-57.6%,ER+30.3%)。延长暴露组与标准组之间的 pCR 率无显著差异。在抗 HER2 治疗的延长阶段,获得了更好的临床反应结果。添加内分泌治疗并未提高 pCR 率。延长抗 HER2 治疗或添加内分泌治疗未发现安全性问题。
本研究证实了 lapatinib、曲妥珠单抗和紫杉醇治疗每个 ER-和 ER+HER2+患者亚组的治疗效果。需要开发进一步的策略和工具,特别是针对 luminal HER2 疾病。