Division of Endocrinology, Diabetes and Metabolism, Department of Medicine, University of Wisconsin, 1685 Highland Avenue, Madison, WI, 53705, USA; William S. Middleton Memorial Veterans Hospital, 2500 Overlook Terrace, Madison, WI 53705, USA.
Division of General Surgery, Department of Surgery, 600 Highland Avenue, University of Wisconsin, Madison, WI, 53705, USA; Division of Bariatric and Gastrointestinal Surgery, Department of Surgery, Virginia Commonwealth University, 1200 East Broad Street, Richmond, VA, 23298, USA.
Mol Metab. 2018 Mar;9:15-27. doi: 10.1016/j.molmet.2017.12.011. Epub 2018 Jan 31.
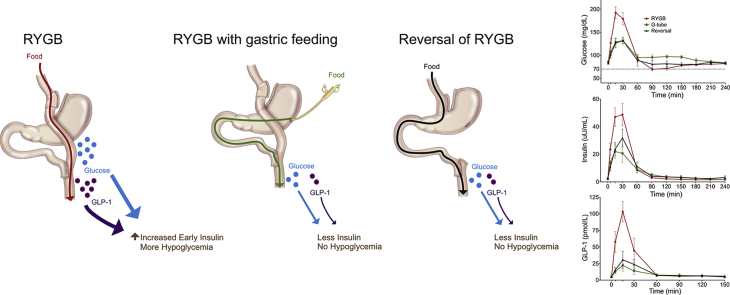
Postprandial hypoglycemia is an infrequent but disabling complication of Roux-en-Y gastric bypass (RYGB) surgery. Controversy still exists as to whether the postprandial hyperinsulinemia observed is due to inherent changes in pancreatic β-cell mass or function or to reversible alterations caused by RYGB anatomy. We aimed to determine if gastric feeding or reversal of RYGB would normalize postprandial glucose and hormone excursions in patients with symptomatic hypoglycemia.
We completed a prospective study of six patients with severe symptomatic RYGB hypoglycemia who underwent RYGB reversal. An additional subject without hypoglycemia who underwent RYGB reversal was also studied prospectively. Mixed meal tolerance testing (MTT) was done orally (RYGB anatomy), via gastrostomy tube in the excluded stomach in the setting of RYGB, and several months after RYGB reversal.
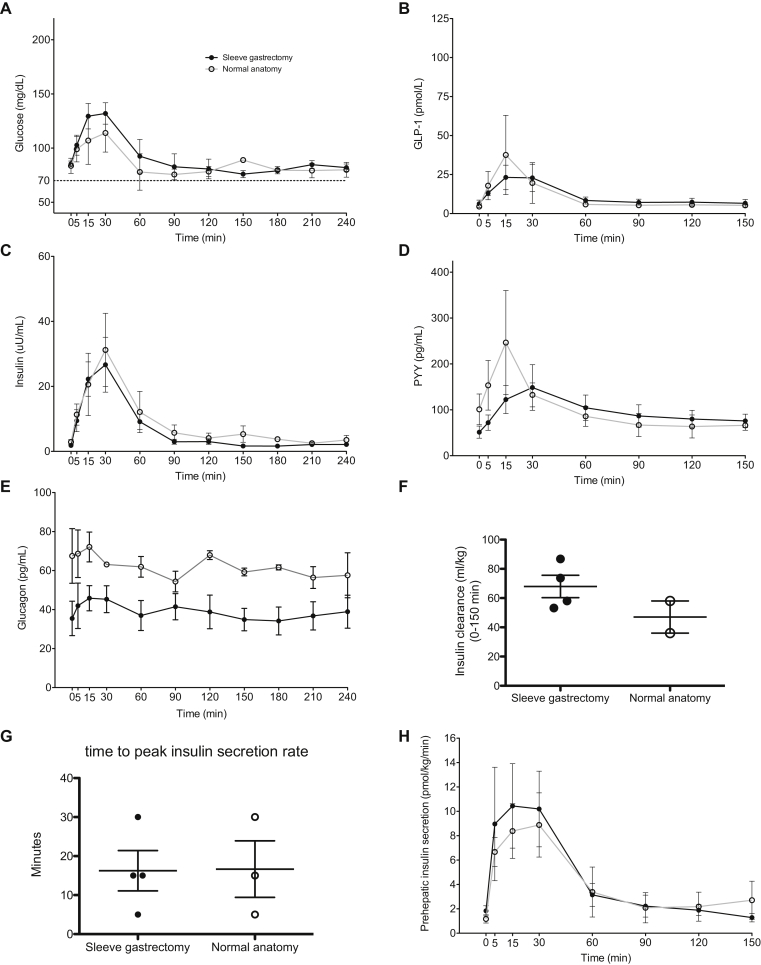
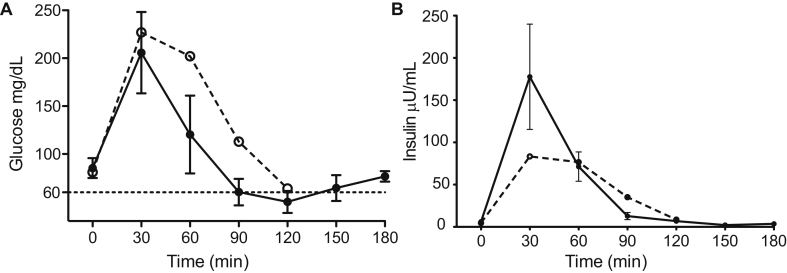
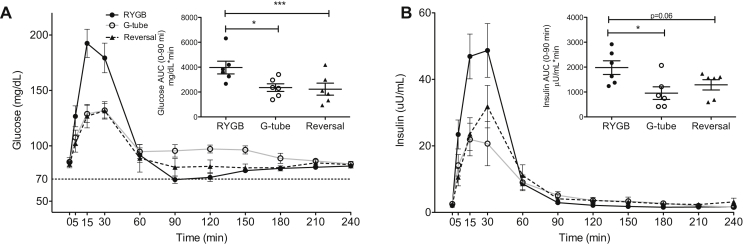
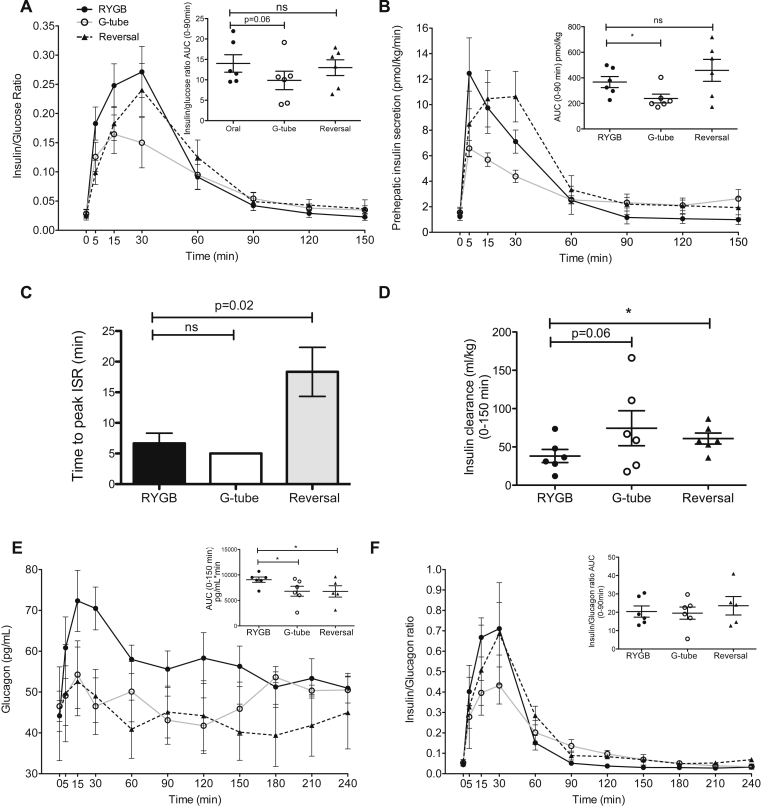
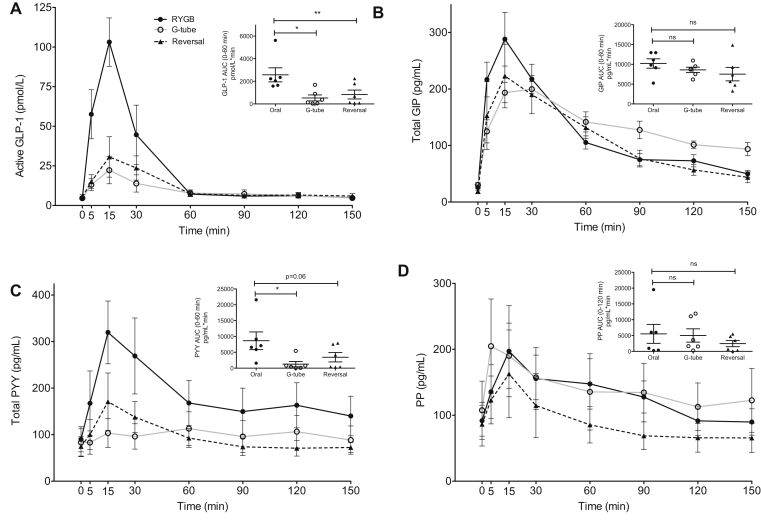
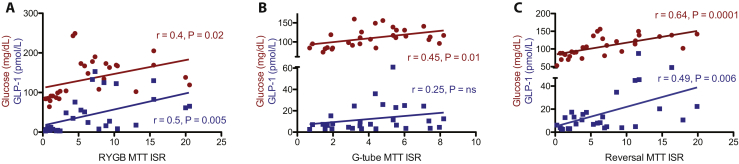
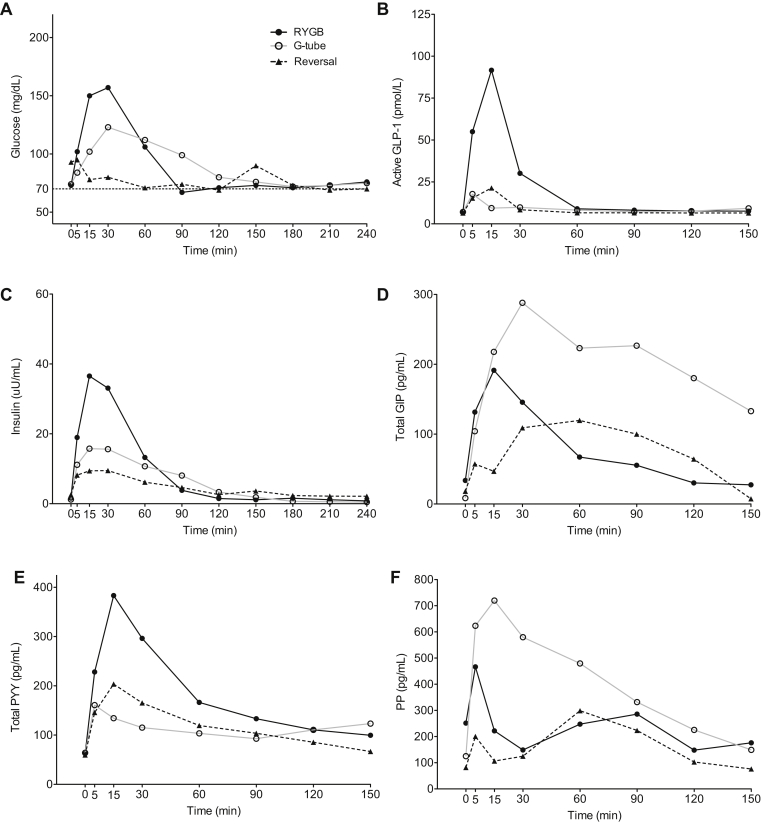
All subjects reported symptomatic improvement of hypoglycemia after reversal of RYGB. Weight gain after reversal was moderate and variable. Postprandial glucose, insulin, and GLP-1 excursions were significantly diminished with gastric feeding and after reversal. Insulin secretion changed proportional to glucose levels and insulin clearance increased after reversal. Glucagon/insulin ratios were similar throughout study. We further compared the impact of modified sleeve gastrectomy reversal surgery to those with restoration of complete stomach and found no significant differences in weight regain or in postprandial glucose or hormone levels.
Reversal of RYGB is an effective treatment option for severe postprandial hypoglycemia. The pathophysiology of this disorder is primarily due to RYGB anatomy resulting in altered glucose, gut, and pancreatic hormone levels and decreased insulin clearance, rather than inherent β-cell hyperplasia or hyperfunction.
餐后低血糖是 Roux-en-Y 胃旁路(RYGB)手术后一种罕见但使人衰弱的并发症。关于所观察到的餐后高胰岛素血症是由于胰腺β细胞质量或功能的固有变化,还是由于 RYGB 解剖结构的可逆改变引起,目前仍存在争议。我们旨在确定胃饲或 RYGB 逆转是否会使有症状性低血糖患者的餐后血糖和激素水平恢复正常。
我们对六例因严重 RYGB 低血糖而接受 RYGB 逆转的患者进行了前瞻性研究。另外一位没有低血糖的接受 RYGB 逆转的患者也进行了前瞻性研究。通过口服(RYGB 解剖结构)、通过 RYGB 中排除的胃中的胃饲管进行混合餐耐量试验(MTT),以及在 RYGB 逆转后几个月进行。
所有患者在 RYGB 逆转后报告低血糖症状改善。逆转后的体重增加适度且变化不定。胃饲和 RYGB 逆转后,餐后血糖、胰岛素和 GLP-1 水平明显降低。胰岛素分泌随血糖水平而变化,胰岛素清除率在逆转后增加。胰高血糖素/胰岛素比值在整个研究过程中相似。我们进一步比较了改良袖状胃切除术逆转手术与恢复完整胃的影响,发现体重恢复、餐后血糖或激素水平无显著差异。
RYGB 逆转是治疗严重餐后低血糖的有效选择。这种疾病的病理生理学主要是由于 RYGB 解剖结构导致的葡萄糖、肠道和胰腺激素水平改变以及胰岛素清除率降低,而不是固有β细胞增生或功能亢进。