Rodríguez-Caulo Emiliano A, Guijarro-Contreras Ana, Otero-Forero Juan, Mataró María José, Sánchez-Espín Gemma, Guzón Arantza, Porras Carlos, Such Miguel, Ordóñez Antonio, Melero-Tejedor José María, Jiménez-Navarro Manuel
UGC Área del Corazón. Servicio de Cirugía Cardiovascular y Cardiología. Hospital Universitario Virgen de la Victoria de Málaga, Spain. Fundación Pública Andaluza para la Investigación de Málaga en Biomedicina y Salud (FIMABIS). Universidad de Málaga. Spain. CIBERCV Enfermedades Cardiovasculares, Instituto de Salud Carlos III, Madrid, Spain.
UGC Área del Corazón, Servicio de Cirugía Cardiovascular, Hospital Universitario Virgen del Rocío de Sevilla, Red de Investigación Cardiovascular (RIC), Instituto de Salud Carlos III, Madrid, Spain.
Trials. 2018 Feb 17;19(1):114. doi: 10.1186/s13063-018-2486-x.
During the last decade, the use of ministernotomy in cardiac surgery has increased. Quality of life and patient satisfaction after ministernotomy have never been compared to conventional full sternotomy in randomised trials. The aim of the study is to determine if this minimally invasive approach improves quality of life, satisfaction and clinical morbimortality outcomes.
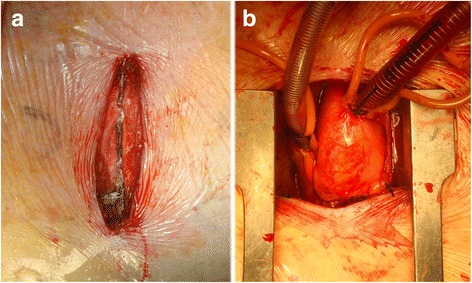
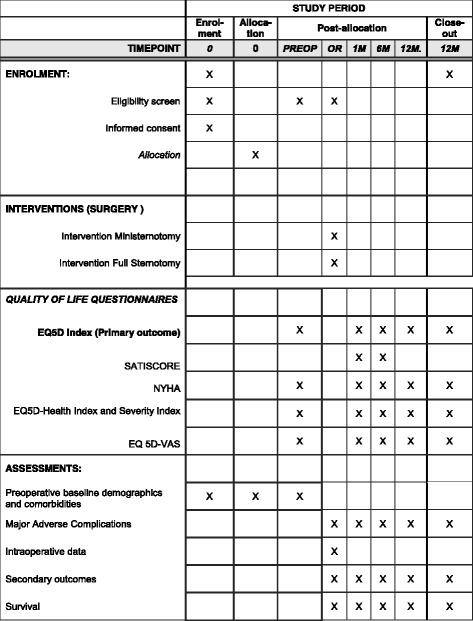
METHODS/DESIGN: The QUALITY-AVR trial is a single-blind, single-centre, independent, and pragmatic randomised clinical trial comparing ministernotomy ("J" shaped upper hemisternotomy toward right 4th intercostal space) to full sternotomy in patients with isolated severe aortic stenosis scheduled for elective aortic valve replacement. One hundred patients will be randomised in a 1:1 computational fashion. Sample size was determined for the primary end point with alpha error of 0.05 and with power of 90% in detecting differences between intervention groups of ≥ 0.10 points in change from baseline quality of life Questionnaire EuroQOL-index (EQ-5D-5 L®), measured at 1, 6 or 12 months. Secondary endpoints are: the differences in change from other baseline EQ-5D-5 L® utilities (visual analogue scale, Health Index and Severity Index), cardiac surgery specific satisfaction questionnaire (SATISCORE®), a combined safety endpoint of four major adverse complications at 1 month (all-cause mortality, acute myocardial infarction, neurologic events and acute renal failure), bleeding through drains within the first 24 h, intubation time, postoperative hospital and intensive care unit length of stay, transfusion needs during the first 72 h and 1-year survival rates. Clinical follow up is scheduled at baseline, 1, 6, and 12 months after randomization. All clinical outcomes are recorded following the Valve Academic Research Consortium 2 criteria.
The QUALITY-AVR trial aims to test the hypothesis that ministernotomy improves quality of life, satisfaction and clinical outcomes in patients referred for isolated aortic valve replacement. Statistically significant differences favouring ministernotomy could modify the surgical "gold standard" for aortic stenosis surgery, and subsequently the need to change the control group in transcatheter aortic valve implantation trials. Recruitment started on 18 March 2016. In November 2017, 75 patients were enrolled.
ClinicalTrials.gov , NCT02726087 . Registered on 13 March 2016.
在过去十年中,心脏手术中微创胸骨切开术的使用有所增加。在随机试验中,微创胸骨切开术后的生活质量和患者满意度从未与传统的全胸骨切开术进行过比较。本研究的目的是确定这种微创方法是否能改善生活质量、满意度和临床病死率结局。
方法/设计:QUALITY-AVR试验是一项单盲、单中心、独立的实用随机临床试验,比较微创胸骨切开术(“J”形上半胸骨切开术至右侧第四肋间)与全胸骨切开术,用于计划进行择期主动脉瓣置换的孤立性严重主动脉瓣狭窄患者。100名患者将以1:1的计算方式随机分组。根据主要终点确定样本量,α错误为0.05,检测干预组之间从基线生活质量欧洲五维健康量表指数(EQ-5D-5L®)变化≥0.10分的差异的检验效能为90%,在1、6或12个月时测量。次要终点包括:其他基线EQ-5D-5L®效用(视觉模拟量表、健康指数和严重程度指数)的变化差异、心脏手术特异性满意度问卷(SATISCORE®)、1个月时四项主要不良并发症的综合安全终点(全因死亡率、急性心肌梗死、神经系统事件和急性肾衰竭)、术后24小时内引流管引流量、插管时间、术后住院和重症监护病房住院时间、术后72小时内输血需求以及1年生存率。临床随访计划在随机分组后的基线、1、6和12个月进行。所有临床结局均按照瓣膜学术研究联盟2标准记录。
QUALITY-AVR试验旨在检验以下假设:微创胸骨切开术可改善计划进行孤立性主动脉瓣置换患者的生活质量、满意度和临床结局。支持微创胸骨切开术的具有统计学意义的差异可能会改变主动脉瓣狭窄手术的外科“金标准”,并随后改变经导管主动脉瓣植入试验中的对照组。招募工作于2016年3月18日开始。2017年11月,已招募75名患者。
ClinicalTrials.gov,NCT02726087。于2016年3月1日注册。