Yoshioka Kaoru, Ohmori Katsuya, Iwasaki Soshi, Takahashi Kazunobu, Sato Akemi, Nakata Hiromasa, Miyamoto Atsushi, Yamakage Michiaki
1Division of Hospital Pharmacy, Sapporo Medical University, South1, West16, Chuo-ku, Sapporo-city, Hokkaido Japan.
3Department of Anesthesiology, Sapporo Medical University, South1, West16, Chuo-ku, Sapporo-city, Hokkaido Japan.
JA Clin Rep. 2017;3(1):35. doi: 10.1186/s40981-017-0092-7. Epub 2017 Jun 12.
Warfarin, a widely used anticoagulant, interacts with various agents used in palliative care, such as oxycodone, morphine, acetaminophen, and non-steroidal anti-inflammatory drugs (NSAIDs); however, there are no reports of its interaction with methadone. We report a case of a patient receiving warfarin when methadone was introduced for pain control with monitoring of the prothrombin time-international normalized ratio (PT-INR) and deduced the pharmacological background.
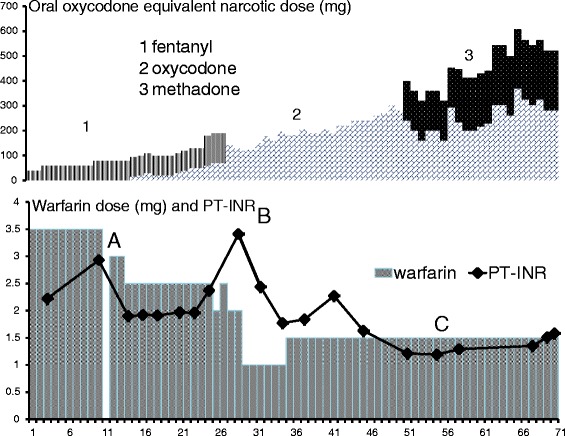
A 60-year-old male was emergently admitted to our university hospital for the sudden onset of severe back pain. Abdominal CT imaging revealed that the vertebral body of the ninth thoracic vertebra was occupied by bone metastasis and crushed, which caused his back pain. He received warfarin 3.5 mg/day for atrial fibrillation and tapentadol 100 mg p.o. daily for pain relief. The prothrombin time-international normalized ratio (PT-INR) was maintained at >2.2. The patient's history included diabetes mellitus and hypertension, but his laboratory test was unremarkable with the exception that his eGFR was 34 ml/min.Initially, a fentanyl dermal patch was used instead of tapentadol to avoid interactions with warfarin. We started concomitant administration of oxycodone and 2.4 g/day of acetaminophen while monitoring the PT-INR because acetaminophen increased the PT-INR to 2.93. A continuous intravenous infusion of oxycodone was introduced, in increments of the dose, resulting in an increase of the PT-INR to 3.41, which is required to reduce the dose of warfarin to 1.5 mg. Because of the lack of effective pain relief, methadone was introduced and the dose was gradually increased. The PT-INR was not changed and the dose of warfarin was not changed. An infusion of oxycodone and oral methadone was used to allow the patient to walk in his room, and he was later transferred to the palliative hospital.
In an oral warfarinized patient, methadone seemed to undergo different metabolism than oxycodone. When warfarin and methadone are used together, we have to consider their interaction by comparing the competitive inhibition of CYP2C9 to the induction of CYP3A4 by methadone, because CYP3A4 metabolize various drugs including oxycodone.
华法林是一种广泛使用的抗凝剂,可与姑息治疗中使用的各种药物相互作用,如羟考酮、吗啡、对乙酰氨基酚和非甾体抗炎药(NSAIDs);然而,尚无其与美沙酮相互作用的报道。我们报告了一例在引入美沙酮控制疼痛时正在接受华法林治疗的患者病例,并监测了凝血酶原时间-国际标准化比值(PT-INR),并推断了其药理学背景。
一名60岁男性因突发严重背痛紧急入住我院。腹部CT成像显示,第九胸椎椎体被骨转移瘤占据并受压,导致其背痛。他因房颤接受3.5毫克/天的华法林治疗,并口服100毫克的曲马多用于止痛。凝血酶原时间-国际标准化比值(PT-INR)维持在>2.2。患者有糖尿病和高血压病史,但实验室检查除估算肾小球滤过率(eGFR)为34毫升/分钟外无异常。最初,使用芬太尼透皮贴剂代替曲马多以避免与华法林相互作用。在监测PT-INR的同时,我们开始联合使用羟考酮和2.4克/天的对乙酰氨基酚,因为对乙酰氨基酚使PT-INR升高至2.93。开始持续静脉输注羟考酮,并逐步增加剂量,导致PT-INR升高至3.41,这需要将华法林剂量减至1.5毫克。由于疼痛缓解效果不佳,引入了美沙酮并逐渐增加剂量。PT-INR未改变,华法林剂量也未改变。使用羟考酮输注和口服美沙酮使患者能够在病房内行走,随后他被转至姑息治疗医院。
在口服华法林的患者中,美沙酮的代谢似乎与羟考酮不同。当华法林和美沙酮一起使用时,我们必须通过比较美沙酮对CYP2C9的竞争性抑制与对CYP3A4的诱导作用来考虑它们的相互作用,因为CYP3A4可代谢包括羟考酮在内的多种药物。