Department of Tumor Biology, Institute for Cancer Research, Oslo University Hospital, Oslo, Norway.
Inserm-U1245, UNIROUEN, Normandie Univ, Normandy Centre for Genomic and Personalized Medicine, Rouen, France.
BMC Med Genet. 2018 Feb 20;19(1):26. doi: 10.1186/s12881-018-0533-9.
The genetic mechanisms for families who meet the clinical criteria for Lynch syndrome (LS) but do not carry pathogenic variants in the mismatch repair (MMR) genes are still undetermined. We aimed to study the potential contribution of genes other than MMR genes to the biological and clinical characteristics of Norwegian families fulfilling Amsterdam (AMS) criteria or revised Bethesda guidelines.
The Hereditary Cancer Biobank of the Norwegian Radium Hospital was interrogated to identify individuals with a high risk of developing colorectal cancer (CRC) for whom no pathogenic variants in MMR genes had been found in routine diagnostic DNA sequencing. Forty-four cancer susceptibility genes were selected and analyzed by using our in-house designed TruSeq amplicon-based assay for targeted sequencing. RNA splicing- and protein-dedicated in silico analyses were performed for all variants of unknown significance (VUS). Variants predicted as likely to affect splicing were experimentally analyzed by resorting to minigene assays.
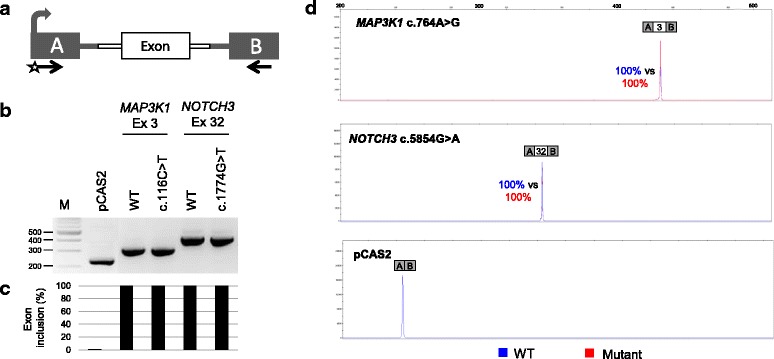
We identified a patient who met the revised Bethesda guidelines and carried a likely pathogenic variant in CHEK2 (c.470 T > C, p.I157T). In addition, 25 unique VUS were identified in 18 individuals, of which 2 exonic variants (MAP3K1 c.764A > G and NOTCH3 c.5854G >A) were analyzed in the minigene splicing assay and found not to have an effect on RNA splicing.
Among high-risk CRC patients that fulfill the AMS criteria or revised Bethesda guidelines, targeted gene sequencing identified likely pathogenic variant and VUS in other genes than the MMR genes (CHEK2, NOTCH3 and MAP3K1). Our study suggests that the analysis of genes currently excluded from routine molecular diagnostic screens may confer cancer susceptibility.
符合林奇综合征(LS)临床标准但 MMR 基因中未携带致病性变异的家族的遗传机制仍未确定。我们旨在研究除 MMR 基因以外的基因对符合阿姆斯特丹(AMS)标准或修订后的贝塞斯达指南的挪威家族的生物学和临床特征的潜在贡献。
挪威镭医院遗传性癌症生物库被查询,以确定那些常规诊断 DNA 测序未发现 MMR 基因致病性变异但患有结直肠癌(CRC)风险较高的个体。选择 44 个癌症易感性基因,并使用我们内部设计的 TruSeq 扩增子靶向测序来分析。对所有意义不明的变异(VUS)进行 RNA 剪接和蛋白质专用的计算机分析。对于预测可能影响剪接的变异,通过 resorting 到 minigene 测定来进行实验分析。
我们发现了一位符合修订后的贝塞斯达指南的患者,携带 CHEK2 中的可能致病性变异(c.470T > C,p.I157T)。此外,在 18 个人中发现了 25 个独特的 VUS,其中 2 个外显子变异(MAP3K1 c.764A > G 和 NOTCH3 c.5854G >A)在 minigene 剪接测定中进行了分析,并未发现对 RNA 剪接有影响。
在符合 AMS 标准或修订后的贝塞斯达指南的高风险 CRC 患者中,靶向基因测序在 MMR 基因以外的基因中发现了可能的致病性变异和 VUS(CHEK2、NOTCH3 和 MAP3K1)。我们的研究表明,分析目前排除在常规分子诊断筛查之外的基因可能会导致癌症易感性。