Taramasso Lucia, Di Biagio Antonio, Bovis Francesca, Nicolini Laura Ambra, Antinori Andrea, Milazzo Laura, Sollima Salvatore, Gubertini Guido, Niero Fosca, Saracino Annalisa, Bruno Raffaele, Borghi Vanni, Montagnani Francesca, Cattelan Annamaria, Hasson Hamid, Taliani Gloria, D'Arminio Monforte Antonella, Mastroianni Claudio, Di Perri Giovanni, Bigoni Sara, Puoti Massimo, Spinetti Angiola, Gori Andrea, Boffa Nicola, Cacopardo Bruno, Giacometti Andrea, Parruti Giustino, Vullo Vincenzo, Chirianni Antonio, Teti Elisabetta, Pasquazzi Caterina, Segala Daniela, Andreoni Massimo
University of Genova (DISSAL), Infectious Diseases Clinic, Policlinico Hospital San Martino, Genova, Italy.
Infectious Diseases Clinic, Policlinico Hospital San Martino, Genova, Italy.
PLoS One. 2018 Feb 20;13(2):e0192627. doi: 10.1371/journal.pone.0192627. eCollection 2018.
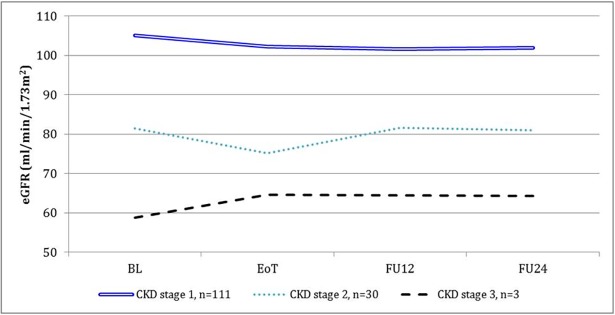
The renal function is a key-issue in HIV/HCV co-infected patients, nevertheless, it has not established so far whether HCV treatment with new direct acting agents could impact on estimated glomerular filtration rate (eGFR) variations. In the present work, we examined the real-life data on renal function that have been prospectively collected in the SIMIT compassionate-use program of ombitasvir/paritaprevir/ritonavir plus dasabuvir (OBV/PTV/r + DSV) in 144 HIV/HCV genotype 1 co-infected patients. The population was 74% male, 30.5% in CDC stage C, with median age of 52 years (48.0-56.5) and median liver stiffness of 7.8 kPa (6.7-9.2). Median baseline eGFR was 102.0 (90.8-108.1), changing to 99.8 (83.5-104.8) at the end of treatment (EoT), and 100.0 (87.3-105.6) 12 weeks after the EoT (FU12), p<0.0001. No patient had grade 3-4 increase of creatinine. At EoT 60/144 (41.7%) patients had ≥ 5% reduction in their eGFR, confirmed at FU12 in 39/60 (65.0%) cases. Longer duration of HCV infection (cut-off 12.9 years), lower HCV-RNA viral load (cut-off 1,970,160 IU/ml) and lower platelet count (cut-off 167,000 x106/L) were significantly associated with eGFR decline at logistic analysis (adjOR 2.9, 95%CI 1.0-8.8, p = 0.05; adjOR 3.5, 95%CI 1.2-10.4, p = 0.02; adjOR 2.8, 95%CI 1.1-6.8, p = 0.03, respectively). After repeating the analysis throughout a mixed model, a higher eGFR decline was highlighted in patients concomitantly treated with tenofovir (p = 0.0001), ribavirin (p = 0.0001), or integrase inhibitors (p <0.0001), with longer duration of HIV (p = 0.0002) and HCV infection (p = 0.035), lower baseline HCV RNA (p <0.0001), previous HCV treatment (p<0.0001), and older age (p<0.0001). In conclusion, our study confirms a good renal safety profile of OBV/PTV/r + DSV treatment in HIV/HCV patients, and the median decline of 2 ml/min in eGFR, albeit statistically significant, is of doubtful clinical significance. The role of aging, concomitant therapies and duration of HIV/HCV infection needs to be further investigated.
肾功能是HIV/HCV合并感染患者的一个关键问题,然而,迄今为止尚未明确使用新型直接作用抗病毒药物进行HCV治疗是否会影响估计肾小球滤过率(eGFR)的变化。在本研究中,我们检查了在ombitasvir/paritaprevir/ritonavir联合dasabuvir(OBV/PTV/r + DSV)的SIMIT同情用药项目中前瞻性收集的144例HIV/HCV基因1型合并感染患者的肾功能实际数据。该人群中男性占74%,30.5%处于美国疾病控制与预防中心(CDC)C期,中位年龄为52岁(48.0 - 56.5岁),中位肝脏硬度为7.8 kPa(6.7 - 9.2)。基线eGFR中位数为102.0(90.8 - 108.1),治疗结束时(EoT)变为99.8(83.5 - 104.8),EoT后12周(FU12)为100.0(87.3 - 105.6),p<0.0001。没有患者肌酐升高至3 - 4级。在EoT时,60/144(41.7%)的患者eGFR下降≥5%,在FU12时,39/60(65.0%)的病例得到确认。在逻辑分析中,HCV感染持续时间较长(截断值为12.9年)、HCV - RNA病毒载量较低(截断值为1,970,160 IU/ml)和血小板计数较低(截断值为167,000×10⁶/L)与eGFR下降显著相关(校正比值比分别为2.9,95%置信区间1.0 - 8.8,p = 0.05;校正比值比3.5,95%置信区间1.2 - 10.4,p = 0.02;校正比值比2.8,95%置信区间1.1 - 6.8,p = 0.03)。在通过混合模型重复分析后,同时接受替诺福韦(p = 0.0001)、利巴韦林(p = 0.0001)或整合酶抑制剂(p <0.0001)治疗的患者中,eGFR下降更为明显,HIV(p = 0.0002)和HCV感染持续时间更长(p = 0.035)、基线HCV RNA较低(p <0.