Kamali Parisa, Ricci Joseph A, Curiel Daniel A, Cohen Justin B, Chattha Anmol, Rakhorst Hinne A, Lee Bernard T, Lin Samuel J
Division of Plastic and Reconstructive Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Mass.; and Division of Plastic and Reconstructive Surgery, Medisch Spectrum Twente, Enschede, The Netherlands.
Plast Reconstr Surg Glob Open. 2018 Jan 12;6(1):e1552. doi: 10.1097/GOX.0000000000001552. eCollection 2018 Jan.
By eliminating economic hurdles, the Women's Health and Cancer Rights Act of 1998 represented a paradigm shift in the availability of breast reconstruction. Yet, studies report disparities among Medicare-insured women. These studies do not account for the inherent differences in age and comorbidities between a younger privately insured and an older Medicare population. We examined immediate breast reconstruction (IBR) utilization between a matched pre- and post-Medicare population.
Using the Nationwide Inpatient Sample database (1992-2013), breast cancer patients undergoing IBR were identified. To minimize confounding medical variables, 64-year-old privately insured women were compared with 66-year-old Medicare-insured women. Demographic data, IBR rates, and complication rates were compared. Trend over time was plotted for both cohorts.
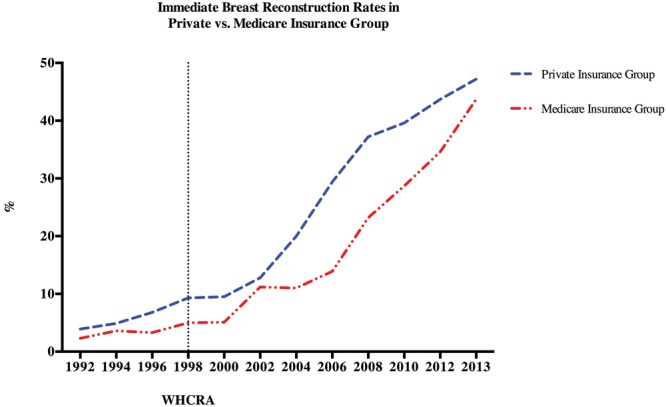
A total of 21,402 64-year-old women and 25,568 66-year-old women were included. Both groups were well matched in terms of demographic type of reconstruction and complication rates. 72.3% of 64-year-old and 71.2 of % 66-year-old women opted for mastectomy. Of these, 25.5% ( = 3,941) of 64-year-old privately insured and 17.7% ( = 3,213) of 66-year-old Medicare-insured women underwent IBR ( < 0.01). During the study period, IBR rates increased significantly in both cohorts in a similar cohort.
This study demonstrates significant increasing IBR rates in both cohorts. Moreover, after an initial slower upward trend, after a decade, IBR in 66-year-old Medicare-insured women approached similar rates of breast reconstruction among those with private insurance. Trends in unilateral versus bilateral mastectomy are also seen.
1998年的《妇女健康与癌症权利法案》消除了经济障碍,代表了乳房重建可及性方面的范式转变。然而,研究报告了医疗保险参保女性之间的差异。这些研究没有考虑年轻的私人保险参保女性和老年医疗保险人群在年龄和合并症方面的固有差异。我们研究了医疗保险参保前后匹配人群之间即刻乳房重建(IBR)的使用情况。
利用全国住院样本数据库(1992 - 2013年),识别接受IBR的乳腺癌患者。为尽量减少混杂的医学变量,将64岁的私人保险参保女性与66岁的医疗保险参保女性进行比较。比较人口统计学数据、IBR率和并发症发生率。绘制了两个队列随时间的趋势图。
共纳入21402名64岁女性和25568名66岁女性。两组在重建的人口统计学类型和并发症发生率方面匹配良好。64岁女性中有72.3%、66岁女性中有71.2%选择了乳房切除术。其中,64岁的私人保险参保女性中有25.5%(n = 3941)、66岁的医疗保险参保女性中有17.7%(n = 3213)接受了IBR(P < 0.01)。在研究期间,两个队列中的IBR率均显著上升,且上升趋势相似。
本研究表明两个队列中的IBR率均显著上升。此外,在最初上升趋势较缓之后,十年后,66岁的医疗保险参保女性的IBR率接近私人保险参保女性的乳房重建率。还观察到单侧与双侧乳房切除术的趋势。