Fontaine Denys, Santucci Serena, Lanteri-Minet Michel
Department of Neurosurgery, CHU de Nice, Université Cote d'Azur, Nice, France.
Université Cote d'Azur, FHU INOVPAIN, CHU de Nice, Nice, France.
J Pain Res. 2018 Feb 16;11:375-381. doi: 10.2147/JPR.S129641. eCollection 2018.
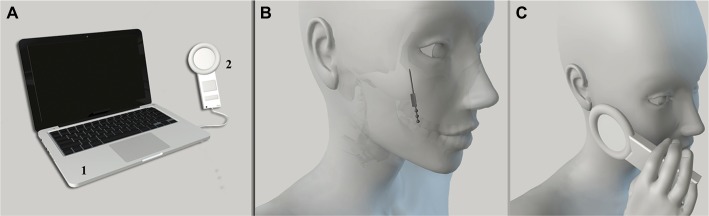
Cluster headache (CH) is a primary headache and considered as one of the worst pains known to man. The sphenopalatine ganglion (SPG) plays a pivotal role in cranial autonomic symptoms associated with pain. Lesioning procedures involving the SPG and experimental acute SPG stimulation have shown some degree of efficacy with regard to CH. A neuromodulation device, chronically implanted in the pterygopalatine fossa, has been specifically designed for acute on-demand SPG stimulation. In a pilot placebo-controlled study in 28 patients suffering from refractory chronic CH, alleviation of pain was achieved in 67.1% of full stimulation-treated attacks compared to 7% of sham stimulation-treated attacks (<0.0001). Long-term results (24 months; 33 patients) confirmed the efficacy of SPG stimulation as an abortive treatment for CH attacks. Moreover, 35% of the patients observed a >50% reduction in attack frequency, suggesting that repeated use of SPG stimulation might act as a CH-preventive treatment. Globally, 61% of the patients were acute responders, frequency responders, or both, and 39% did not respond to SPG stimulation. The safety of SPG microstimulator implantation procedure was evaluated in a cohort of 99 patients; facial sensory disturbances were observed in 67% of the patients (46% of them being transient), transient allodynia in 3%, and infection in 5%. SPG stimulation appears as a promising innovative, efficient, and safe therapeutic solution for patients suffering from severe CH. It has shown its efficacy in aborting CH attacks compared to placebo stimulation, suggesting that it is particularly adapted for CH patients who are not sufficiently improved by abortive treatments such as sumatriptan and oxygen. However, further studies comparing SPG stimulation with standard abortive and/or preventive CH treatments will be necessary to define more precisely its place within the management of severe chronic and/or episodic CH.
丛集性头痛(CH)是一种原发性头痛,被认为是人类已知的最严重的疼痛之一。蝶腭神经节(SPG)在与疼痛相关的颅神经自主症状中起关键作用。涉及SPG的损伤手术和实验性急性SPG刺激在CH方面已显示出一定程度的疗效。一种长期植入翼腭窝的神经调节装置专门设计用于急性按需SPG刺激。在一项针对28例难治性慢性CH患者的安慰剂对照试验研究中,与假刺激治疗的发作(7%)相比,完全刺激治疗的发作中有67.1%实现了疼痛缓解(<0.0001)。长期结果(24个月;33例患者)证实了SPG刺激作为CH发作的一种中止治疗的疗效。此外,35%的患者发作频率降低了>50%,这表明重复使用SPG刺激可能起到预防CH的作用。总体而言,61%的患者是急性反应者、频率反应者或两者皆是,39%的患者对SPG刺激无反应。在一组99例患者中评估了SPG微刺激器植入手术的安全性;67%的患者出现面部感觉障碍(其中46%为短暂性),3%出现短暂性异常性疼痛,5%出现感染。SPG刺激似乎是一种有前景的、创新的、有效且安全的治疗方案,适用于患有严重CH的患者。与安慰剂刺激相比,它已显示出中止CH发作的疗效,这表明它特别适用于那些未通过舒马曲坦和吸氧等中止治疗得到充分改善的CH患者。然而,需要进一步比较SPG刺激与标准中止和/或预防性CH治疗的研究,以便更准确地确定其在严重慢性和/或发作性CH管理中的地位。