Cardiac Imaging Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Korean J Intern Med. 2019 May;34(3):510-518. doi: 10.3904/kjim.2017.152. Epub 2018 Mar 5.
BACKGROUND/AIMS: Although the association between intrapulmonary shunt (IPS) and liver cirrhosis is clear, data of repeated contrast echocardiography (CE) before and after liver transplantation (LT) to evaluate factors associated with IPS are limited.
Hand-agitated saline was used for CE and, by assessing left-chamber opacification, IPS was classified as grade 0 to 4. Grade 3/4 constituted significant IPS and hepatopulmonary syndrome (HPS) was defined as significant IPS with the arterial partial pressure of oxygen < 70 mmHg.
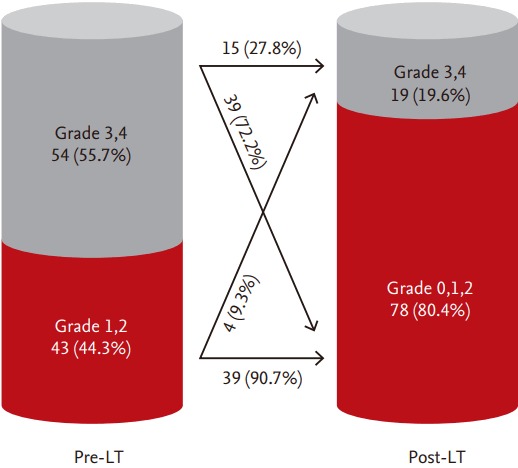
Before LT, 253 patients underwent CE and the frequency of significant IPS and HPS were 44% (n = 112) and 7% (n = 17), respectively. Child-Pugh score (odds ratio [OR], 1.345; 95% confidence interval [CI], 1.090 to 1.660; p = 0.006) and arterial oxygen content (OR, 0.838; 95% CI, 0.708 to 0.991; p = 0.039) were independent determinants of significant IPS, whereas direct bilirubin (OR, 1.076; 95% CI, 1.012 to 1.144; p = 0.019) was the only variable associated with HPS. Among 153 patients who underwent successful LT, repeated CE was performed in 97 (63%), which showed significant reductions in IPS grade (from 2.6 ± 1.0 to 1.2 ± 1.3, p < 0.001) and the prevalence of significant IPS (from 56% to 20%, p = 0.038). After adjustment for pre-LT IPS grade, time from LT to repeated CE presented negative linear relationship with post-LT IPS grade (r 2 = 0.366, p < 0.001) and was the only determinant of post-LT IPS grade (OR, 1.009; 95% CI, 1.003 to 1.014; p = 0.004).
Repeated CE is useful to evaluate intrapulmonary vascular change before and after LT. Reversal of IPS after successful LT is time-dependent and follow-up duration should be considered for accurate assessment of IPS after LT.
背景/目的:虽然肺内分流(IPS)与肝硬化之间的关联是明确的,但关于移植前和移植后重复对比超声心动图(CE)评估与 IPS 相关的因素的数据有限。
采用手动搅拌生理盐水进行 CE,并通过评估左心室混浊程度,将 IPS 分为 0 至 4 级。3/4 级构成显著 IPS,肝肺综合征(HPS)定义为显著 IPS 伴动脉血氧分压 < 70mmHg。
LT 前,253 例患者接受了 CE,显著 IPS 和 HPS 的频率分别为 44%(n=112)和 7%(n=17)。Child-Pugh 评分(比值比 [OR],1.345;95%置信区间 [CI],1.090 至 1.660;p=0.006)和动脉血氧含量(OR,0.838;95%CI,0.708 至 0.991;p=0.039)是显著 IPS 的独立决定因素,而直接胆红素(OR,1.076;95%CI,1.012 至 1.144;p=0.019)是唯一与 HPS 相关的变量。在 153 例成功接受 LT 的患者中,97 例(63%)进行了重复 CE,结果显示 IPS 分级显著降低(从 2.6±1.0 降至 1.2±1.3,p<0.001),显著 IPS 的发生率从 56%降至 20%(p=0.038)。在校正 LT 前 IPS 分级后,LT 至重复 CE 的时间与 LT 后 IPS 分级呈负线性关系(r 2=0.366,p<0.001),是 LT 后 IPS 分级的唯一决定因素(OR,1.009;95%CI,1.003 至 1.014;p=0.004)。
重复 CE 可用于评估 LT 前后肺血管变化。成功 LT 后 IPS 的逆转是时间依赖性的,应考虑随访时间,以准确评估 LT 后的 IPS。