Tomov Marko, Tou Kevin, Winkel Rose, Puffer Ross, Bydon Mohamad, Nassr Ahmad, Huddleston Paul, Yaszemski Michael, Currier Bradford, Freedman Brett
Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USA.
Department of Orthopedic Surgery, United States Army, Landstuhl, Germany.
Asian Spine J. 2018 Feb;12(1):85-93. doi: 10.4184/asj.2018.12.1.85. Epub 2018 Feb 7.
Retrospective case-control study using prospectively collected data.
Evaluate the impact of liposomal bupivacaine (LB) on postoperative pain management and narcotic use following standardized single-level low lumbar transforaminal lumbar interbody fusion (TLIF).
Poor pain control after surgery has been linked with decreased pain satisfaction and increased economic burden. Unfortunately, opioids have many limitations and side effects despite being the primary treatment of postoperative pain. LB may be a form of pre-emptive analgesia used to reduce the use of postoperative narcotics as evidence in other studies evaluating its use in single-level microdiskectomies.
The infiltration of LB subcutaneously during wound closure was performed by a single surgeon beginning in July 2014 for all single-level lumbar TLIF spinal surgeries at Landstuhl Regional Medical Center. This cohort was compared against a control cohort of patients who underwent the same surgery by the same surgeon in the preceding 6 months. Statistical analysis was performed on relevant variables including: morphine equivalents of narcotic medication used (primary outcome), length of hospitalization, Visual Analog Scale pain scores, and total time spent on a patient-controlled analgesia (PCA) pump.
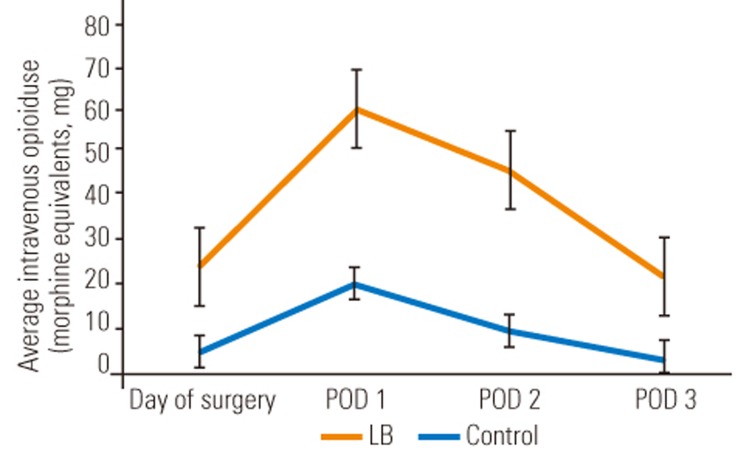
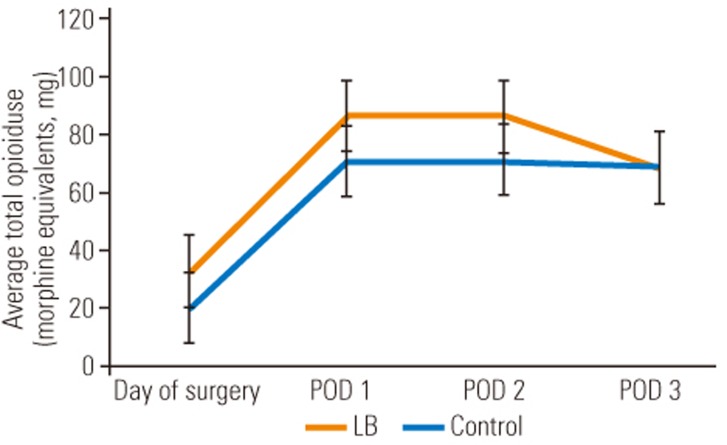
A total of 30 patients were included in this study; 16 were in the intervention cohort and 14 were in the control cohort. The morphine equivalents of intravenous narcotic use postoperatively were significantly less in the LB cohort from day of surgery to postoperative day 3. Although the differences lost their statistical significance, the trend remained for total (oral and intravenous) narcotic consumption to be lower in the LB group. The patients who received the study intervention required an acute pain service consult less frequently (62.5% in LB cohort vs. 78.6% in control cohort). The amount of time spent on a PCA pump in the LB group was 31 hours versus 47 hours in the control group (=0.1506).
Local infiltration of LB postoperatively to the subcutaneous tissues during closure following TLIF significantly decreased the amount of intravenous narcotic medication required by patients. Well-powered prospective studies are still needed to determine optimal dosing and confirm benefits of LB on total narcotic consumption and other measures of pain control following major spinal surgery.
使用前瞻性收集的数据进行回顾性病例对照研究。
评估脂质体布比卡因(LB)对标准化单节段低位腰椎椎间孔腰椎椎体间融合术(TLIF)后疼痛管理和麻醉药物使用的影响。
术后疼痛控制不佳与疼痛满意度降低和经济负担增加有关。不幸的是,尽管阿片类药物是术后疼痛的主要治疗方法,但它有许多局限性和副作用。在其他评估其在单节段显微椎间盘切除术应用的研究中,LB可能是一种用于减少术后麻醉药物使用的超前镇痛形式。
自2014年7月起,由一名外科医生对兰施图尔地区医疗中心所有单节段腰椎TLIF脊柱手术患者在伤口闭合时进行LB皮下浸润。该队列与前6个月由同一名外科医生进行相同手术的患者对照组进行比较。对相关变量进行统计分析,包括:使用的麻醉药物吗啡当量(主要结果)、住院时间、视觉模拟评分疼痛评分以及患者自控镇痛(PCA)泵使用的总时间。
本研究共纳入30例患者;16例在干预队列,14例在对照队列。从手术当天到术后第3天,LB队列术后静脉使用麻醉药物的吗啡当量显著低于对照组。尽管差异失去统计学意义,但LB组总(口服和静脉)麻醉药物消耗量较低的趋势仍然存在。接受研究干预的患者需要急性疼痛服务咨询的频率较低(LB队列中为62.5%,对照组中为78.6%)。LB组PCA泵使用时间为31小时,而对照组为47小时(P = 0.1506)。
TLIF术后伤口闭合时将LB局部浸润至皮下组织显著减少了患者所需静脉麻醉药物的量。仍需要有充分说服力的前瞻性研究来确定最佳剂量,并证实LB对脊柱大手术后总麻醉药物消耗量和其他疼痛控制指标的益处。