Department of Preventive and Emergency Cardiology, Sechenov First Moscow State Medical University, Moscow, Russia.
A.I. Evdokimov Moscow State University of Medicine and Dentistry, Moscow, Russia.
Adv Ther. 2018 Mar;35(3):341-352. doi: 10.1007/s12325-018-0681-5. Epub 2018 Mar 5.
Heart rate (HR) reduction is an integral part of antianginal therapy, but many patients do not reach the guideline-recommended target of less than 60 bpm despite high use of beta-blockers (BB). Failure to uptitrate BB doses may be partly to blame. To explore other options for lowering HR and improving angina control, CONTROL-2 was initiated to compare the efficacy and tolerability of the combination of BBs with ivabradine versus uptitration of BBs to maximal tolerated dose, in patients with stable angina.
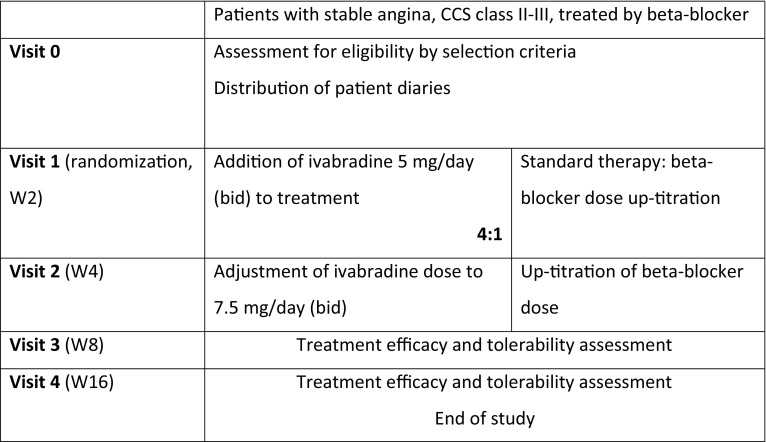
This multicenter, open, randomized study included 1104 patients with Canadian Cardiovascular Society (CCS) class II or III stable angina, in sinus rhythm, and on background stable treatment with non-maximal recommended doses of BBs. Consecutive patients were allocated to ivabradine + BB or BB uptitration in a 4:1 ratio.
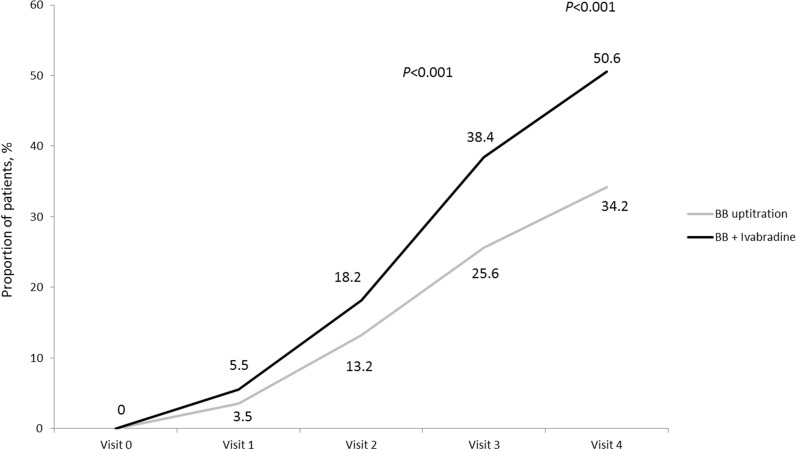
At the end of the study (week 16), addition of ivabradine to BB treatment and BB uptitration resulted in reduction in HR (61 ± 6 vs. 63 ± 8 bpm; p = 0.001). At week 16, significantly more patients on ivabradine + BB were in CCS class I than with BB uptitration (37.1% vs. 28%; p = 0.017) and significantly more patients were angina-free (50.6% vs. 34.2%; p < 0.001). Patient health status based on the visual analogue scale (VAS) was also better in the ivabradine + BB group. Adverse events (AEs) were significantly more common with BB uptitration than with the ivabradine + BB combination (18.4% vs. 9.4%, p < 0.001).
In patients with stable angina, combination therapy with ivabradine + BB demonstrated good tolerability, safety, and more pronounced clinical improvement, compared to BB uptitration.
ISRCTN30654443.
Servier.
心率(HR)降低是抗心绞痛治疗的一个组成部分,但许多患者尽管大量使用β受体阻滞剂(BB),仍未达到低于 60 bpm 的指南推荐目标。未能增加 BB 剂量可能是部分原因。为了探索降低 HR 和改善心绞痛控制的其他选择,启动了 CONTROL-2 研究,以比较 BB 联合伊伐布雷定与增加 BB 剂量至最大耐受剂量在稳定型心绞痛患者中的疗效和耐受性。
这是一项多中心、开放、随机研究,纳入了 1104 例加拿大心血管学会(CCS)Ⅱ级或Ⅲ级稳定型心绞痛、窦性心律和在背景稳定治疗下接受非最大推荐剂量 BB 的患者。连续患者按 4:1 的比例随机分配至伊伐布雷定+BB 或 BB 剂量递增。
研究结束时(第 16 周),BB 治疗中添加伊伐布雷定和 BB 剂量递增导致 HR 降低(61±6 vs. 63±8 bpm;p=0.001)。第 16 周时,伊伐布雷定+BB 组的 CCS 分级Ⅰ级患者显著多于 BB 剂量递增组(37.1% vs. 28%;p=0.017),无心绞痛患者显著更多(50.6% vs. 34.2%;p<0.001)。基于视觉模拟量表(VAS)的患者健康状况也在伊伐布雷定+BB 组更好。与伊伐布雷定+BB 组相比,BB 剂量递增组的不良事件(AE)更为常见(18.4% vs. 9.4%;p<0.001)。
在稳定型心绞痛患者中,与 BB 剂量递增相比,伊伐布雷定+BB 联合治疗具有良好的耐受性、安全性和更明显的临床改善。
ISRCTN30654443。
Servier。