Department of Radiology, Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, 200092, China.
Department of Radiotherapy, Ruijin Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, 200025, China.
Cancer Med. 2018 Apr;7(4):1160-1169. doi: 10.1002/cam4.1417. Epub 2018 Mar 13.
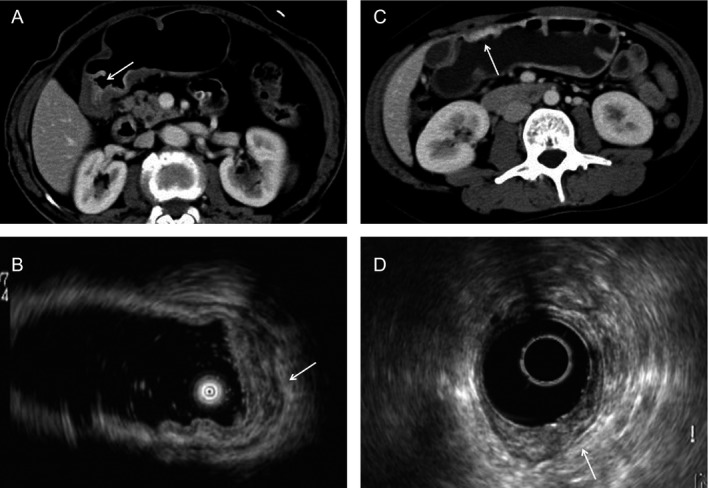
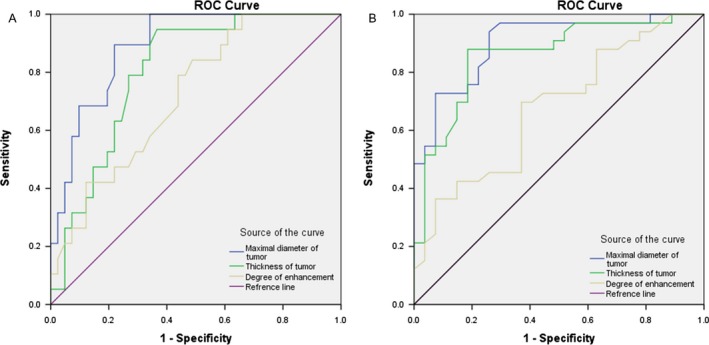
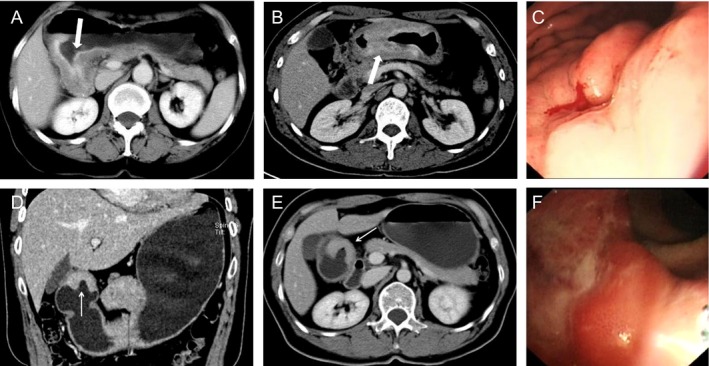
Signet ring cell carcinoma (SRC) of the stomach is a histological type based on microscopic characteristics. SRC's clinicopathological characteristics and prognosis are still controversial. Our study is to describe the clinicopathological features and multidetector computed tomography (MDCT) findings of patients with SRC of the stomach in comparison with nonsignet ring cell adenocarcinoma (NSRC). We retrospectively analyzed data from 241 patients who had undergone curative gastrectomy, including 62 SRC and 179 NSRC. Clinicopathological outcomes and MDCT findings were evaluated, and we investigated whether these variables were correlated with histopathological type. In early gastric carcinoma, patients with SRC were younger (50.2 vs. 60.2 years; P = 0.000) and more likely to be observed in the middle and lower third stomach (P = 0.010). Early SRC had a tendency to be confined to the mucosa (82.1%). There were significant differences in degree of enhancement between early SRC and NSRC on MDCT imaging (P < 0.001). In advanced gastric carcinoma, SRC was more likely to be stage T3-4 (100%). SRC patients had thicker tumors (P = 0.001) and a higher frequency of diffusely infiltrative gross appearance (P < 0.001). SRC was more likely to have high-degree contrast enhancement than were NSRC (P = 0.001). The maximal diameter of SRC tumor on MDCT imaging correlated with lymph node metastasis (sensitivity 93.9%, specificity 74.1%) and serosal invasion (sensitivity 89.5%, specificity 78.0%) of SRC. In conclusion, SRC differs significantly from NSRC in clinicopathological features at presentation. MDCT could help differentiate advanced gastric SRC from NSRC based on the thickened stomach wall, high-degree contrast enhancement, and a higher frequency of diffusely infiltrative gross appearance, particularly in combination.
胃的印戒细胞癌 (SRC) 是一种基于显微镜特征的组织学类型。SRC 的临床病理特征和预后仍存在争议。我们的研究旨在描述与非印戒细胞腺癌 (NSRC) 相比,胃 SRC 患者的临床病理特征和多排螺旋 CT (MDCT) 表现。我们回顾性分析了 241 例接受根治性胃切除术患者的数据,其中 SRC 为 62 例,NSRC 为 179 例。评估了临床病理结局和 MDCT 表现,并研究了这些变量是否与组织病理学类型相关。在早期胃癌中,SRC 患者更年轻(50.2 岁 vs. 60.2 岁;P=0.000),更可能发生在中下部胃(P=0.010)。早期 SRC 倾向于局限于黏膜(82.1%)。早期 SRC 和 NSRC 之间在 MDCT 成像上的增强程度存在显著差异(P<0.001)。在进展期胃癌中,SRC 更可能处于 T3-4 期(100%)。SRC 患者的肿瘤更厚(P=0.001),弥漫浸润性大体外观的发生率更高(P<0.001)。SRC 的高程度对比增强率高于 NSRC(P=0.001)。MDCT 成像上 SRC 肿瘤的最大直径与淋巴结转移(SRC 的灵敏度 93.9%,特异性 74.1%)和浆膜侵犯(SRC 的灵敏度 89.5%,特异性 78.0%)相关。总之,SRC 在临床表现上与 NSRC 有显著差异。MDCT 可以帮助区分进展期胃 SRC 和 NSRC,其依据是增厚的胃壁、高程度的对比增强和弥漫浸润性大体外观的更高发生率,尤其是联合使用时。