Hospital at Home Unit, Tower C, Floor 1 Office 5, La Fe University Hospital, Valencia, Spain & CASPe, Spain.
Department of Pharmacy, La Fe University Hospital, Valencia, Spain, & CASPe, Spain.
J Cachexia Sarcopenia Muscle. 2018 Jun;9(3):444-452. doi: 10.1002/jcsm.12292. Epub 2018 Mar 14.
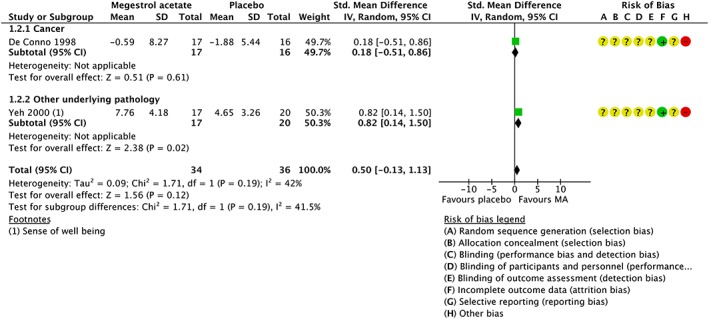
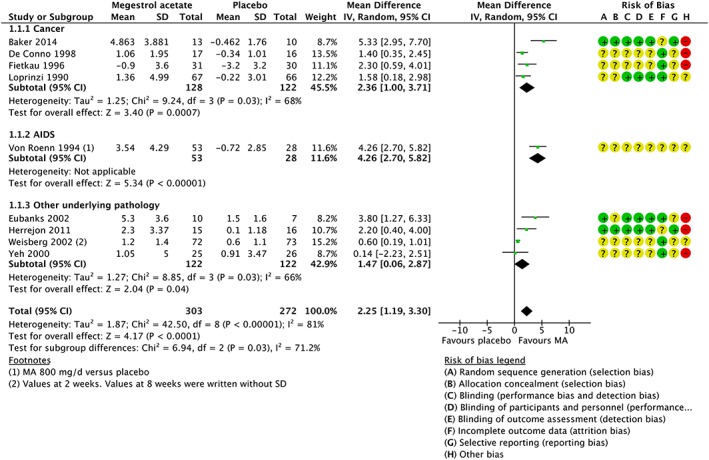
In 1993, megestrol acetate (MA) was approved by the US Food and Drug Administration for the treatment of anorexia, cachexia, or unexplained weight loss in patients with acquired immunodeficiency syndrome. The mechanism by which MA increases appetite is unknown, and its effectiveness for anorexia and cachexia in neoplastic, elderly, and acquired immunodeficiency syndrome patients is under investigation. This is an updated version of a Cochrane systematic review first published in 2005 and later updated in 2013 entitled 'Megestrol acetate for the treatment of anorexia-cachexia syndrome'. MA vs. placebo: in studies where MA was compared with placebo, the overall results showed that MA patients gained weight (mean difference, MD 2.25 kg, 95% CI [1.19, 3.3]) but did not gain quality of life (QOL) (standarized mean difference, SMD 0.5, 95% CI [-0.13, 1.13]), with more adverse events (relative risk, RR 1.46, 95% CI [1.05, 2.04]), but no difference in deaths (RR 1.26, 95% CI [0.70, 2.27]). MA vs. no treatment: MA patients gained weight (MD 1.45 kg, 95% CI [0.15, 2.75]) but did not gain QOL (standardized mean difference 3.89 95% CI [-14, 6.28]). There was no increase in adverse events (RR 0.90, 95% CI [0.39, 2.08]) or deaths (RR 1.01, 95% CI [0.42, 2.45]). MA vs. active drugs: MA patients gained weight (MD 2.5 kg, 95% CI [0.37, 4.64]) but did not gain QOL (MD 0.20 95% CI [-0.02, 0.43]) and did not report an increase in adverse events (RR 1.05 95% CI [0.95, 1.16]) or in deaths (RR 1.53, 95% CI [1.02, 2.29]) Different doses of MA: in studies where lower doses of MA were compared with higher doses of MA, we did not find differences either in weight gain (MD -0.94 kg, 95% CI [-3.33, 1.45]), QOL (MD 0.31 95% CI [-0.19, 0.81]), or adverse events (RR 1.34, 95% CI [0.65, 2.76]). Thus, we cannot reach a conclusion for an optimal dose of MA.
1993 年,美替拉酮(MA)经美国食品和药物管理局批准,用于治疗获得性免疫缺陷综合征患者的厌食、恶病质或不明原因的体重减轻。MA 增加食欲的机制尚不清楚,其在肿瘤、老年和获得性免疫缺陷综合征患者的厌食和恶病质中的疗效仍在研究中。这是 Cochrane 系统评价的更新版本,最初于 2005 年发表,后来于 2013 年更新,题为“美替拉酮治疗厌食-恶病质综合征”。MA 与安慰剂相比:在将 MA 与安慰剂进行比较的研究中,总体结果表明 MA 患者体重增加(平均差异,MD 2.25kg,95%CI[1.19,3.3]),但生活质量(QOL)没有改善(标准化均数差,SMD 0.5,95%CI[-0.13,1.13]),不良事件更多(相对风险,RR 1.46,95%CI[1.05,2.04]),但死亡率无差异(RR 1.26,95%CI[0.70,2.27])。MA 与无治疗相比:MA 患者体重增加(MD 1.45kg,95%CI[0.15,2.75]),但 QOL 无改善(标准均数差 3.89,95%CI[-14,6.28])。不良事件(RR 0.90,95%CI[0.39,2.08])或死亡率(RR 1.01,95%CI[0.42,2.45])均无增加。MA 与活性药物相比:MA 患者体重增加(MD 2.5kg,95%CI[0.37,4.64]),但 QOL 无改善(MD 0.20,95%CI[-0.02,0.43]),不良事件(RR 1.05,95%CI[0.95,1.16])或死亡率(RR 1.53,95%CI[1.02,2.29])均无增加。MA 的不同剂量:在比较 MA 低剂量与高剂量的研究中,我们没有发现体重增加(MD-0.94kg,95%CI[-3.33,1.45])、QOL(MD 0.31,95%CI[-0.19,0.81])或不良事件(RR 1.34,95%CI[0.65,2.76])方面的差异。因此,我们无法确定 MA 的最佳剂量。