Fujio Atsushi, Usuda Masahiro, Ozawa Yohei, Kamiya Kurodo, Nakamura Takanobu, Teshima Jin, Murakami Kazushige, Suzuki On, Miyata Go, Mochizuki Izumi
Department of Gastroenterological Surgery, Iwate Prefectural Central Hospital, Iwate, 020-0066, Japan.
Int J Surg Case Rep. 2017 Nov 21;41:434-437. doi: 10.1016/j.ijscr.2017.11.025. eCollection 2017.
Pseudoaneurysm is a serious complication after pancreatic surgery, which mainly depends on the presence of a preceding pancreatic fistula. Postpancreatectomy hemorrhage following total pancreatectomy is a rare complication due to the absence of a pancreatic fistula. Here we report an unusual case of massive gastrointestinal bleeding due to right hepatic artery (RHA) pseudoaneurysm following total remnant pancreatectomy.
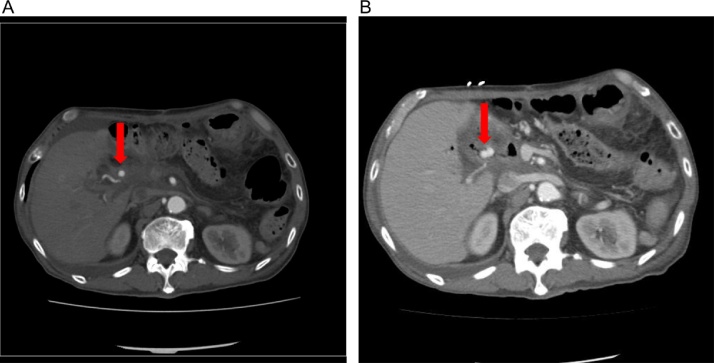
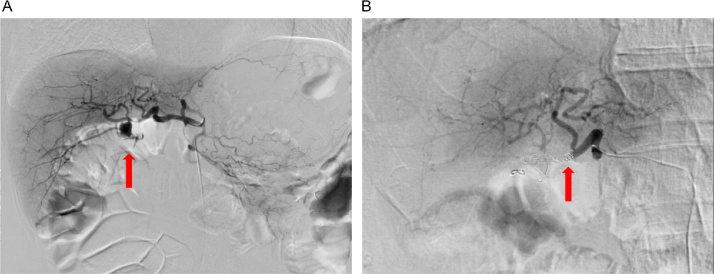
A 75-year-old man was diagnosed with intraductal papillary mucinous carcinoma recurrence following distal pancreatectomy and underwent total remnant pancreatectomy. After discharge, he was readmitted to our hospital with melena because of the diagnosis of gastrointestinal bleeding. Gastrointestinal endoscopy was performed to detect the origin of bleeding, but an obvious bleeding point could not be detected. Abdominal computed tomography demonstrated an expansive growth, which indicated RHA pseudoaneurysm. Emergency angiography revealed gastrointestinal bleeding into the jejunum from the ruptured RHA pseudoaneurysm. Transcatheter arterial embolization was performed; subsequently, bleeding was successfully stopped for a short duration. Because of improvements in his general condition, the patient was discharged.
To date, very few cases have described postpancreatectomy hemorrhage following total remnant pancreatectomy. We suspect that the aneurysm ruptured into the jejunum, possibly because of the scarring and inflammation associated with his two complex surgeries.
Pseudoaneurysm should be considered when the fragility of blood vessels is suspected, despite no history of anastomotic leak and intra-abdominal abscess. Our case also highlighted that detecting gastrointestinal bleeding is necessary to recognize sentinel bleeding if the origin of bleeding is undetectable.
假性动脉瘤是胰腺手术后的一种严重并发症,主要取决于先前是否存在胰瘘。全胰切除术后胰切除术后出血是一种罕见的并发症,因为不存在胰瘘。在此,我们报告一例全胰切除术后因右肝动脉(RHA)假性动脉瘤导致大量胃肠道出血的罕见病例。
一名75岁男性在远端胰腺切除术后被诊断为导管内乳头状黏液性癌复发,并接受了全胰切除术。出院后,因诊断为胃肠道出血,他再次入住我院,出现黑便。进行了胃肠内镜检查以检测出血来源,但未发现明显的出血点。腹部计算机断层扫描显示有扩张性生长,提示为RHA假性动脉瘤。急诊血管造影显示破裂的RHA假性动脉瘤导致空肠出现胃肠道出血。进行了经导管动脉栓塞术;随后,出血在短时间内成功停止。由于患者一般状况有所改善,遂出院。
迄今为止,很少有病例描述全胰切除术后的胰切除术后出血。我们怀疑动脉瘤破裂进入空肠,可能是由于他的两次复杂手术相关的瘢痕形成和炎症。
尽管没有吻合口漏和腹腔内脓肿病史,但当怀疑血管脆弱时,应考虑假性动脉瘤。我们的病例还强调,如果出血来源无法检测到,检测胃肠道出血对于识别哨兵出血是必要的。