Yamada Reiko, Sakuno Takashi, Inoue Hiroyuki, Miura Hiroshi, Takeuchi Toshifumi, Shiono Yasunori, Okuse Hiroaki, Nakamura Misaki, Katsurahara Masaki, Hamada Yasuhiko, Tanaka Kyosuke, Horiki Noriyuki, Takei Yoshiyuki
Department of Gastroenterology and Hepatology, Mie University Hospital, Mie University Graduate School of Medicine, 2-174 Edobashi, Tsu, Mie, 514-8507, Japan.
Department of Endoscopy, Mie University Graduate School of Medicine, Tsu, Japan.
Clin J Gastroenterol. 2018 Aug;11(4):286-290. doi: 10.1007/s12328-018-0848-2. Epub 2018 Mar 15.
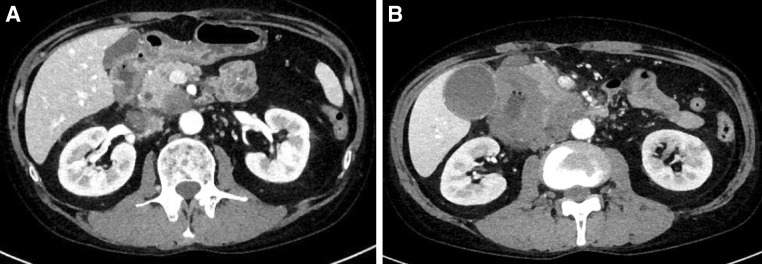
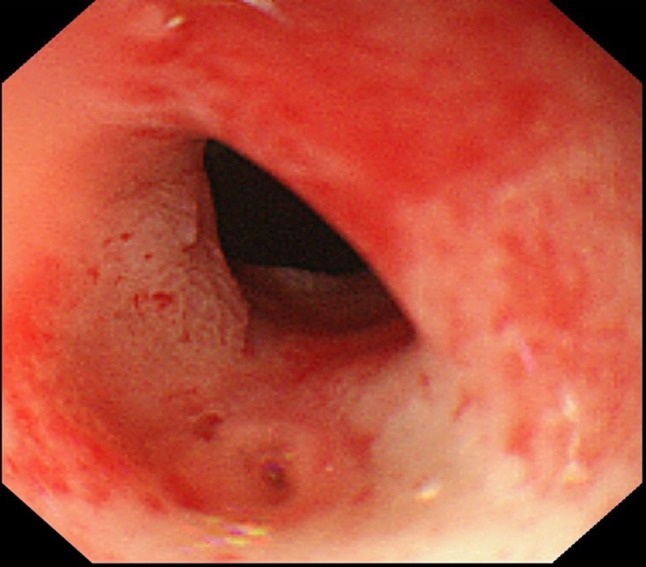
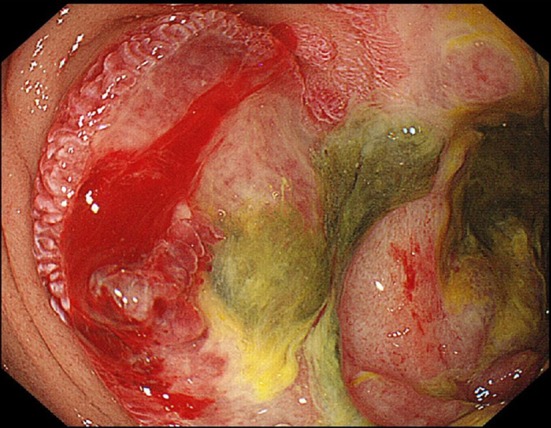
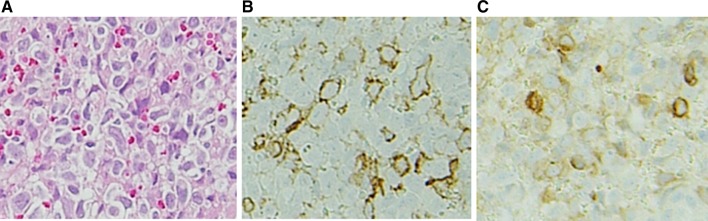
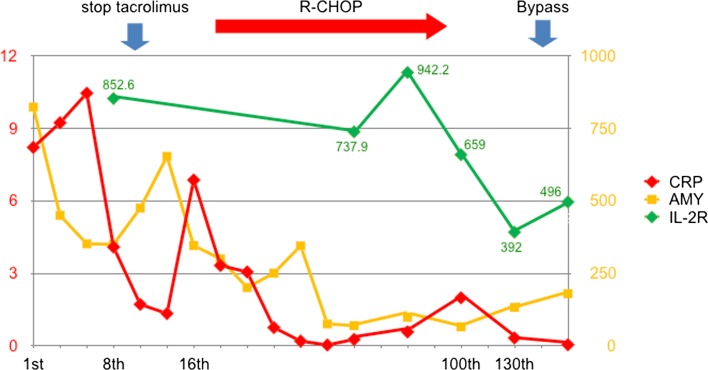
A 49-year-old man was admitted to our hospital with pancreatitis. He was diagnosed with systemic lupus erythematosus at 34 years of age and was being treated with oral tacrolimus (3 mg/day) and predonine (10 mg/day) for the past 15 months. The computed tomography (CT) scan showed the mass lesion had invaded the pancreatic head via thickening of the duodenal wall. Upper gastrointestinal endoscopy showed the all-round ulcerative lesion from the superior duodenal angle to the descending portion. Histological examination confirmed the diagnosis of diffuse large B cell lymphoma (DLBCL). Tacrolimus therapy was stopped due to the possibility of immunodeficiency-related lymphoproliferative disease; however, the lesion did not improve. Consequently, he was administered rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). After six courses of R-CHOP therapy, a partial response was confirmed on CT. One month after the completion of chemotherapy, a gastrojejunal anastomosis was performed because of duodenal stenosis. He has since been well without recurrence. It was difficult to identify the risk factor for DLBCL; therefore, both the disease activity and immunosuppressive therapy should be taken into consideration as carrying a risk. In the present case, the symptom of pancreatitis enabled an early diagnosis of DLBCL.
一名49岁男性因胰腺炎入院。他在34岁时被诊断为系统性红斑狼疮,在过去15个月里一直口服他克莫司(3毫克/天)和泼尼松(10毫克/天)进行治疗。计算机断层扫描(CT)显示肿块病变通过十二指肠壁增厚侵犯了胰头。上消化道内镜检查显示从十二指肠上角到降部有全周溃疡性病变。组织学检查确诊为弥漫性大B细胞淋巴瘤(DLBCL)。由于存在免疫缺陷相关淋巴增殖性疾病的可能性,他克莫司治疗被停止;然而,病变并未改善。因此,给他使用了利妥昔单抗联合环磷酰胺、多柔比星、长春新碱和泼尼松(R-CHOP)。经过六个疗程的R-CHOP治疗后,CT证实有部分缓解。化疗结束后1个月,因十二指肠狭窄进行了胃空肠吻合术。此后他情况良好,未复发。很难确定DLBCL的危险因素;因此,疾病活动和免疫抑制治疗都应被视为有风险因素。在本病例中,胰腺炎症状使得能够早期诊断DLBCL。