International Centre for Eye Health, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Aravind Eye Hospital, Madurai, India; Aravind Medical Research Foundation, Madurai, India.
Am J Ophthalmol. 2018 Jun;190:24-33. doi: 10.1016/j.ajo.2018.03.010. Epub 2018 Mar 14.
To determine cellular features of fungal (FK), Acanthamoeba (AK), and bacterial keratitis (BK) using HRT3 in vivo confocal microscopy (IVCM).
Prospective observational cross-sectional study.
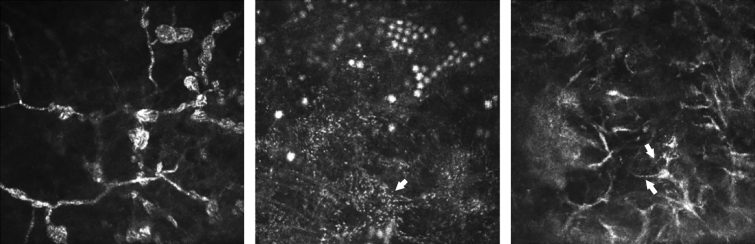
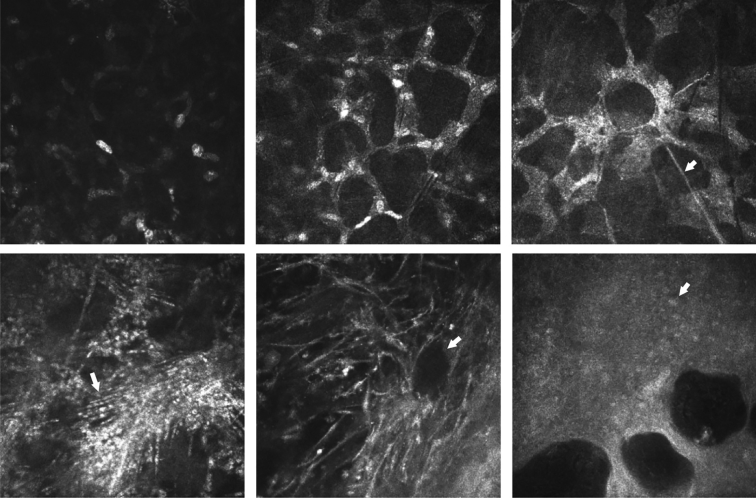
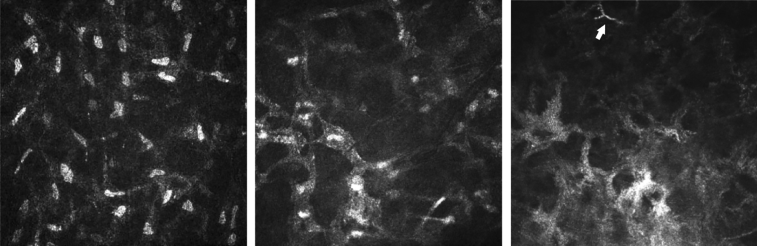
Eligible participants were adults with microbiologically positive FK, AK, or BK, of size ≥ 3 mm, attending Aravind Eye Hospital from February 2012 to February 2013. Exclusion criteria were descemetocele or perforation. At presentation, IVCM imaging was performed, then corneal scrapes were obtained for culture/light microscopy. An experienced grader (masked to microbiology/clinical features) assessed IVCM images for presence/absence of normal keratocyte-like morphology, stellate interconnected cells with/without visible nuclei, dendritiform cells (DFCs), inflammatory cells in a honeycomb distribution, and organism features. Statistical significance was assessed by logistic regression, adjusted for age, sex, ulcer size, and symptom duration. Main outcome measures were presence/absence of IVCM features in FK, AK, BK.
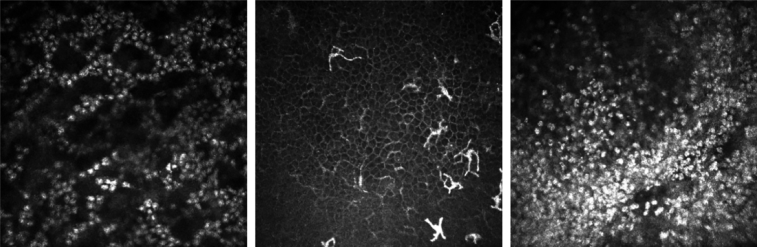
A total of 183 participants had FK, 18 AK, 17 BK. Acanthamoeba appeared as bright spots (16/18, 89%), double-walled cysts (15/18, 83%), or signet rings (3/18, 17%), and often formed clusters after topical steroid use (univariable odds ratio [OR] 9.98, 95% confidence interval [CI] 1.02-97.96, P = .048). BK was associated with bullae in anterior stroma (OR 9.99, 95% CI: 3.11-32.06, P < .001). Honeycomb distribution of anterior stromal inflammatory cells was associated with FK (univariable OR 2.74, 95% CI: 1.01-7.40, P = .047). Aspergillus ulcers were associated with stromal DFCs (OR 11.05, 95% CI: 1.49-82.13, P = .019) and Fusarium ulcers with stellate appearance of interconnected cell processes with nuclei (OR 0.24, 95% CI: 0.09-0.65, P = .005).
Specific cellular and structural features observed using IVCM in microbial keratitis may be associated with organism.
使用共聚焦显微镜(IVCM)确定真菌(FK)、棘阿米巴(AK)和细菌性角膜炎(BK)的细胞特征。
前瞻性观察性横断面研究。
纳入 2012 年 2 月至 2013 年 2 月在阿拉文德眼科医院就诊的微生物学阳性 FK、AK 或 BK 且大小≥3mm 的成年患者。排除标准为角膜后弹力层膨出或穿孔。入组时进行 IVCM 成像,然后进行角膜刮片培养/光学显微镜检查。一位经验丰富的分级员(对微生物学/临床特征进行盲法评估)评估 IVCM 图像是否存在/不存在正常的角膜基质细胞样形态、有/无可见核的星状相互连接的细胞、树突状细胞(DFC)、呈蜂窝状分布的炎症细胞和生物体特征。采用 logistic 回归评估统计学意义,并对年龄、性别、溃疡大小和症状持续时间进行调整。主要观察指标为 FK、AK、BK 中 IVCM 特征的存在/缺失。
共纳入 183 例 FK、18 例 AK、17 例 BK。棘阿米巴表现为亮斑(16/18,89%)、双层囊(15/18,83%)或套环(3/18,17%),且常在外用类固醇使用后形成簇(单变量比值比[OR]9.98,95%置信区间[CI]1.02-97.96,P=0.048)。BK 与前基质中的大疱相关(OR 9.99,95%CI:3.11-32.06,P<0.001)。前基质炎症细胞呈蜂窝状分布与 FK 相关(单变量 OR 2.74,95%CI:1.01-7.40,P=0.047)。曲霉性溃疡与基质 DFC 相关(OR 11.05,95%CI:1.49-82.13,P=0.019),而镰刀菌性溃疡与有核的相互连接细胞突起呈星状外观相关(OR 0.24,95%CI:0.09-0.65,P=0.005)。
微生物角膜炎中使用 IVCM 观察到的特定细胞和结构特征可能与病原体有关。