Xie Sherlly, Hossain Md Jobayer
Biostatistics Core, Nemours Biomedical Research, A I duPont Hospital for Children, Wilmington, DE 19803, United States.
Biostatistics Core, Nemours Biomedical Research, A I duPont Hospital for Children, Wilmington, DE 19803, United States; Department of Applied Economics and Statistics, University of Delaware, Newark, DE 19716, United States.
Cancer Epidemiol. 2018 Jun;54:19-24. doi: 10.1016/j.canep.2018.03.001. Epub 2018 Mar 16.
Acute myeloid leukemia (AML) is a serious disease with complex etiology and marked variation in survival. Known prognostic factors include AML subtypes, age at diagnosis and sex. However, survival outcomes may vary across healthcare systems. In this study, we evaluated the survival patterns in individuals diagnosed with AML at ages 0-24 years in the US and England between prognostic features and across countries.
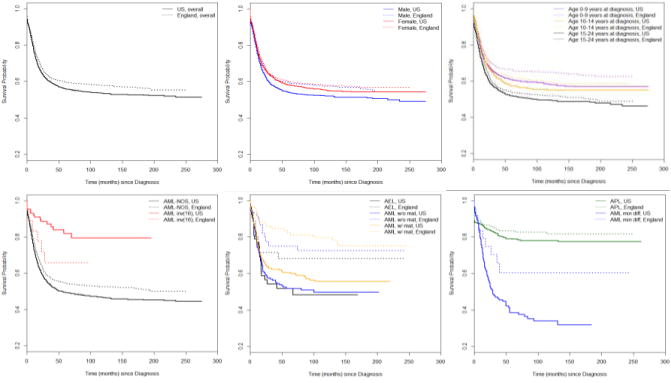
We obtained data on 4387 and 2194 subjects from the US Surveillance Epidemiology and End Result registries and UK National Cancer Data Repository. Subjects were diagnosed and followed in 1995-2014. Kaplan-Meier curve and stratified Cox proportional hazards regression were used in the analysis.
Overall risk of mortality was 23% lower in English patients compared to that in the US patients (adjusted hazard ratio (aHR), 95% confidence Interval (CI): 0.77, 0.71-0.84). Survival difference of similar extent was observed in subgroups of sex and age at diagnosis. However, mortality risks between two countries varied substantially across AML subtypes, especially in AML inv(16) (1.81, 0.61-5.34), AML with minimal differentiation (0.54, 0.25-1.17), AML without maturation (0.38, 0.20-0.74) and AML with maturation (0.52, 0.31-0.86).
Similar to the population trend, mortality risk across sex, age at diagnosis, and most AML subtypes was lower in England. Survival outcome for AML with and without maturation in England was better than the population trend, while that for AML inv(16) was worse. Our findings suggest that future etiologic and policy research may uncover the underlying mechanisms and contribute to closing these morality gaps.
急性髓系白血病(AML)是一种病因复杂、生存情况差异显著的严重疾病。已知的预后因素包括AML亚型、诊断时的年龄和性别。然而,不同医疗体系中的生存结果可能有所不同。在本研究中,我们评估了美国和英国0至24岁AML确诊患者的生存模式,比较了预后特征及两国之间的差异。
我们从美国监测、流行病学和最终结果登记处以及英国国家癌症数据存储库获取了4387名和2194名受试者的数据。这些受试者于1995年至2014年被诊断并接受随访。分析采用Kaplan-Meier曲线和分层Cox比例风险回归。
英国患者的总体死亡风险比美国患者低23%(调整后风险比(aHR),95%置信区间(CI):0.77,0.71 - 0.84)。在性别和诊断时年龄的亚组中也观察到了类似程度的生存差异。然而,两国之间的死亡风险在不同AML亚型中差异很大,尤其是在AML inv(16)(1.81,0.61 - 5.34)、微分化AML(0.54,0.25 - 1.17)、未成熟AML(0.38,0.20 - 0.74)和成熟AML(0.52, 0.31 - 0.8)中。
与总体趋势相似,英国在性别、诊断时年龄以及大多数AML亚型方面的死亡风险较低。英国有成熟和无成熟AML的生存结果优于总体趋势,而AML inv(16)的生存结果则较差。我们的研究结果表明,未来的病因学和政策研究可能会揭示潜在机制,并有助于缩小这些死亡率差距。