International Centre for Diarrhoeal Disease Research, Bangladesh, Dhaka, Bangladesh.
Centers for Disease Control and Prevention, Atlanta, GA, USA.
Lancet Infect Dis. 2018 Jun;18(6):657-665. doi: 10.1016/S1473-3099(18)30113-0. Epub 2018 Mar 20.
Monovalent type 2 oral poliovirus vaccine (mOPV2) and inactivated poliovirus vaccine (IPV) are used to respond to type 2 poliovirus outbreaks. We aimed to assess the effect of two mOPV2 doses on the type 2 immune response by varying the time interval between mOPV2 doses and IPV co-administration with mOPV2.
We did a randomised, controlled, parallel, open-label, non-inferiority, inequality trial at two study clinics in Dhaka, Bangladesh. Healthy infants aged 6 weeks (42-48 days) at enrolment were randomly assigned (1:1:1:1) to receive two mOPV2 doses (each dose consisting of two drops [0·1 mL in total] of about 10 50% cell culture infectious dose of type 2 Sabin strain) at intervals of 1 week, 2 weeks, 4 weeks (standard or control group), or 4 weeks with IPV (0·5 mL of type 1 [Mahoney, 40 D-antigen units], type 2 [MEF-1, 8 D-antigen units], and type 3 [Saukett, 32 D-antigen units]) administered intramuscularly with the first mOPV2 dose. We used block randomisation, randomly selecting blocks of sizes four, eight, 12, or 16 stratified by study sites. We concealed randomisation assignment from staff managing participants in opaque, sequentially numbered, sealed envelopes. Parents and clinic staff were unmasked to assignment after the randomisation envelope was opened. Laboratory staff analysing sera were masked to assignment, but investigators analysing data and assessing outcomes were not. The primary outcome was type 2 immune response measured 4 weeks after mOPV2 administration. The primary modified intention-to-treat analysis included participants with testable serum samples before and after vaccination. A non-inferiority margin of 10% and p=0·05 (one-tailed) was used. This trial is registered at ClinicalTrials.gov, number NCT02643368, and is closed to accrual.
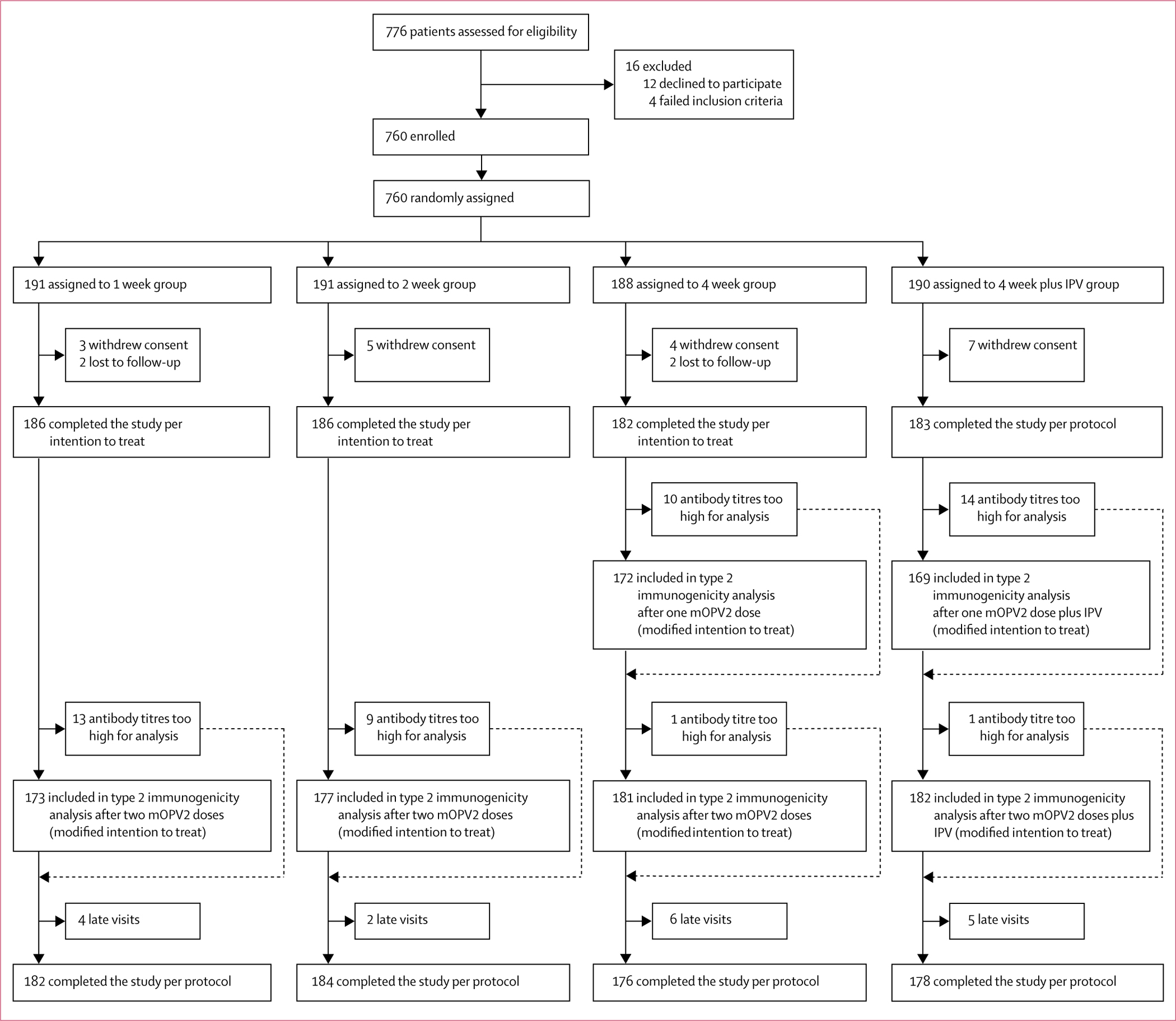
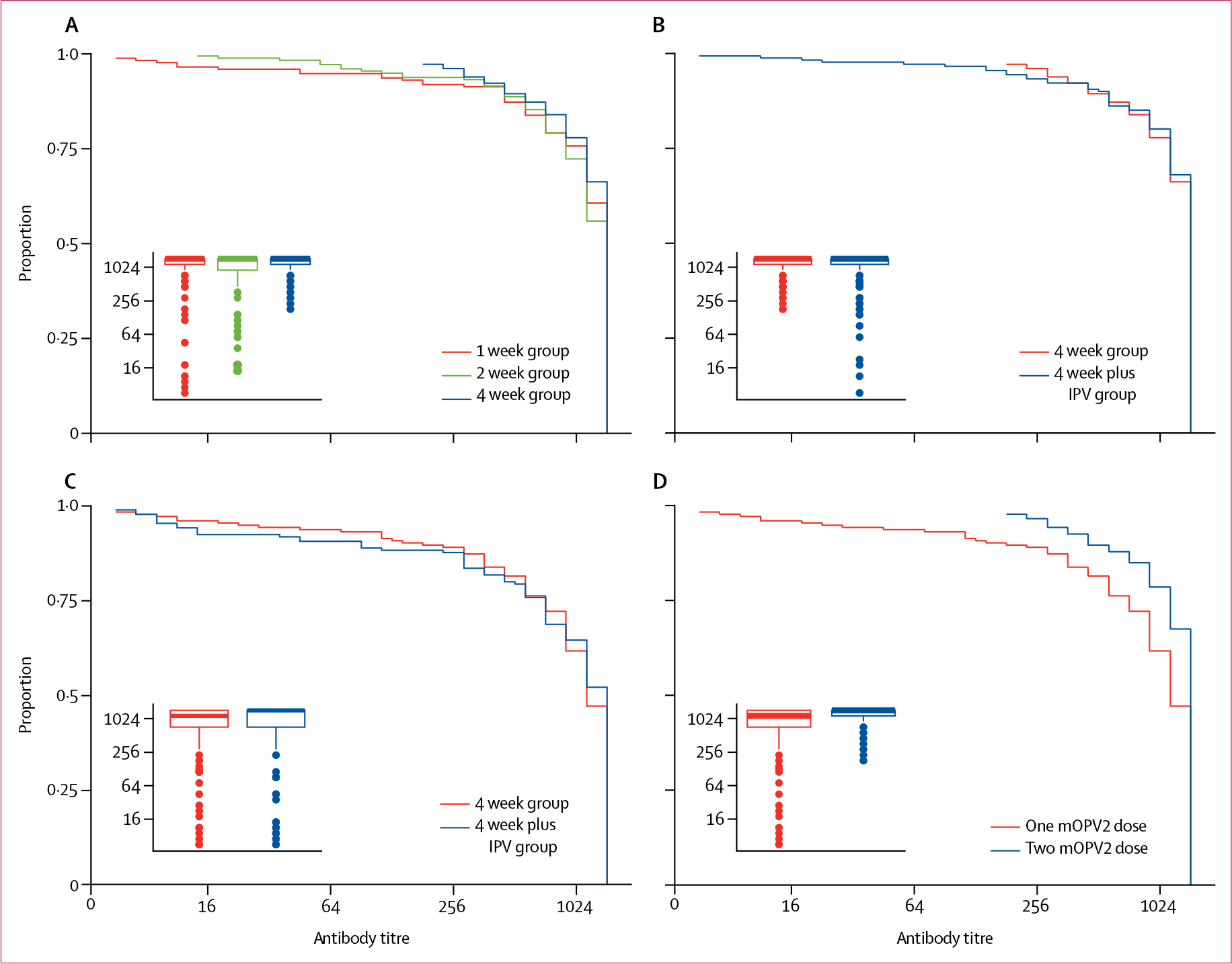
Between Dec 7, 2015, and Jan 5, 2016, we randomly assigned 760 infants to receive two mOPV2 doses at intervals of 1 week (n=191), 2 weeks (n=191), 4 weeks (n=188), or 4 weeks plus IPV (n=190). Immune responses after two mOPV2 doses were observed in 161 (93%) of 173 infants with testable serum samples in the 1 week group, 169 (96%) of 177 in the 2 week group, and 176 (97%) of 181 in the 4 week group. 1 week and 2 week intervals between two mOPV2 doses were non-inferior to 4 week intervals because the lower bound of the absolute differences in the percentage of immune responses were greater than -10% (-4·2% [90% CI -7·9 to -0·4] in the 1 week group and -1·8% [-5·0 to 1·5] in the 2 week group vs the 4 week group). The immune response elicited by two mOPV2 doses 4 weeks apart was not different when IPV was added to the first dose (176 [97%] of 182 infants with IPV vs 176 [97%] of 181 without IPV; p=1·0). During the trial, two serious adverse events (pneumonia; one [1%] of 186 patients in the 1 week group and one [1%] of 182 in the 4 week group) and no deaths were reported; the adverse events were not attributed to the vaccines.
Administration of mOPV2 at short intervals does not interfere with its immunogenicity. The addition of IPV to the first mOPV2 dose did not improve poliovirus type 2 immune response.
US Centers for Disease Control and Prevention.
单价 2 型口服脊髓灰质炎疫苗(mOPV2)和灭活脊髓灰质炎疫苗(IPV)用于应对 2 型脊灰病毒暴发。我们旨在通过改变 mOPV2 剂量与 mOPV2 与 IPV 共同给药之间的时间间隔,评估两种 mOPV2 剂量对 2 型脊灰病毒免疫反应的影响。
我们在孟加拉国达卡的两个研究诊所进行了一项随机、对照、平行、开放性、非劣效性、不平等性试验。入组时年龄为 6 周(42-48 天)的健康婴儿按 1:1:1:1 的比例随机分配(1:1:1:1)接受两种 mOPV2 剂量(每剂各含 2 滴[0·1 mL 总含量]约 10 50%细胞培养 2 型 Sabin 株的感染剂量),间隔 1 周、2 周、4 周(标准或对照组)或 4 周与 IPV(0·5 mL 型 1 [马霍尼,40 D 抗原单位]、型 2 [MEF-1,8 D 抗原单位]和型 3 [Saukett,32 D 抗原单位])肌肉内给药与第一剂 mOPV2 一起。我们使用块随机化,随机选择大小为 4、8、12 或 16 的块,按研究地点分层。我们将随机化分配隐藏在不透明的、顺序编号的、密封的信封中,不让工作人员管理参与者的人员看到。父母和诊所工作人员在打开随机化信封后才知道分配情况。实验室工作人员对血清进行分析时是盲的,但分析数据和评估结果的研究人员不是盲的。主要结局是 mOPV2 给药后 4 周的 2 型免疫反应。主要的改良意向治疗分析包括接种前后有可检测血清样本的参与者。使用 10%的非劣效性边界和 p=0·05(单侧)。这项试验在 ClinicalTrials.gov 注册,编号为 NCT02643368,现已停止入组。
在 2015 年 12 月 7 日至 2016 年 1 月 5 日期间,我们随机分配了 760 名婴儿接受两种 mOPV2 剂量,间隔 1 周(n=191)、2 周(n=191)、4 周(n=188)或 4 周加 IPV(n=190)。在 1 周组中有 173 名婴儿中有可检测的血清样本,其中 161 名(93%)在 2 周组中有 177 名(96%),在 4 周组中有 181 名(97%)。2 剂 mOPV2 之间 1 周和 2 周的间隔不劣于 4 周的间隔,因为免疫反应百分比的绝对差异的下限大于-10%(1 周组为-4·2%[7·9 至-0·4],2 周组为-1·8%[-5·0 至 1·5])与 4 周组相比)。4 周间隔分开接种两剂 mOPV2 时,当第一剂加入 IPV 时,免疫反应没有差异(182 名婴儿中有 186 名接种 IPV 的婴儿与 181 名没有接种 IPV 的婴儿的免疫反应相同;p=1·0)。在试验期间,报告了两例严重不良事件(肺炎;1 周组中有 1 名[1%]婴儿和 4 周组中有 1 名[1%]婴儿)和无死亡病例;不良事件与疫苗无关。
短时间间隔内使用 mOPV2 不会干扰其免疫原性。第一剂 mOPV2 中加入 IPV 并不能改善 2 型脊灰病毒的免疫反应。
美国疾病控制和预防中心。