From the Department of Anesthesiology.
Division of Biomedical Informatics, University of California, San Diego, San Diego, California.
Anesth Analg. 2018 Oct;127(4):1044-1050. doi: 10.1213/ANE.0000000000003342.
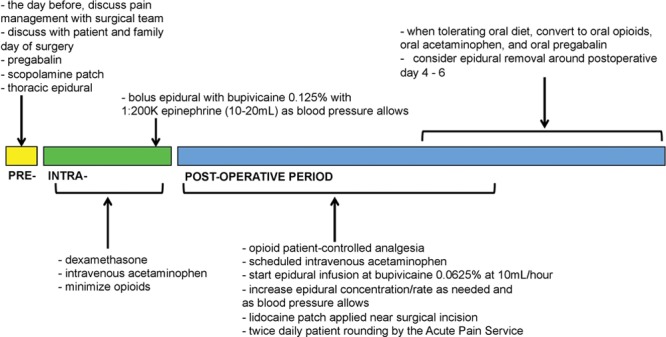
The Acute Pain Service (APS) was initially introduced to optimize multimodal postoperative pain control. The aim of this study was to evaluate the association between the implementation of an APS and postoperative pain management and outcomes for patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC).
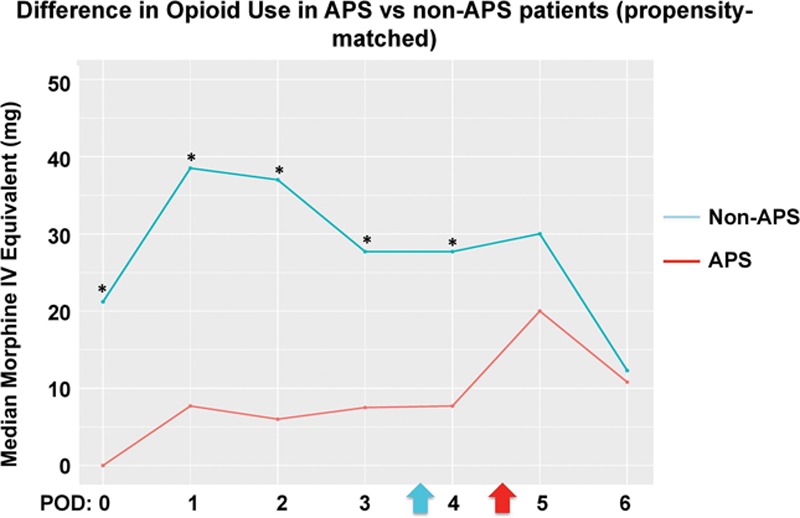
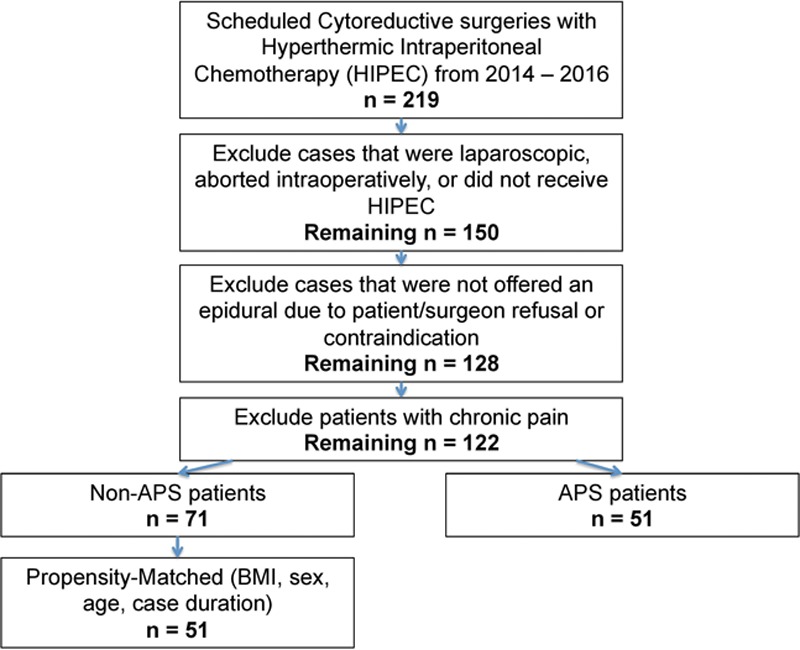
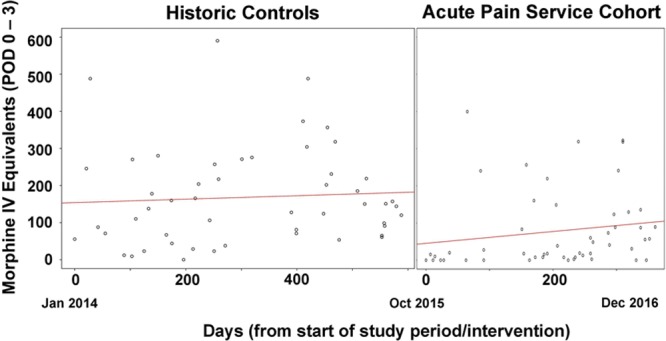
In this propensity-matched retrospective cohort study, we performed a before-after study without a concurrent control group. Outcomes were compared among patients undergoing CRS-HIPEC when APS was implemented versus historical controls (non-APS). The primary objective was to determine if there was a decrease in median total opioid consumption during postoperative days 0-3 among patients managed by the APS. Secondary outcomes included opioid consumption on each postoperative day (0-6), time to ambulation, time to solid intake, and hospital length of stay.
After exclusion, there were a total of 122 patients, of which 51 and 71 were in the APS and non-APS cohort, respectively. Between propensity-matched groups, the median (quartiles) total opioid consumption during postoperative days 0-3 was 27.5 mg intravenous morphine equivalents (MEQs) (7.6-106.3 mg MEQs) versus 144.0 mg MEQs (68.9-238.3 mg MEQs), respectively. The median difference was 80.8 mg MEQs (95% confidence interval, 46.1-124.0; P < .0001). There were statistically significant decreases in time to ambulation and time to solid diet intake in the APS cohort.
After implementing the APS, CRS-HIPEC patients had decreased opioid consumption by >50%, as well as shorter time to ambulation and time to solid intake. Implementation of an APS may improve outcomes in CRS-HIPEC patients.
急性疼痛服务(APS)最初是为了优化多模式术后疼痛控制而引入的。本研究的目的是评估 APS 的实施与行细胞减灭术联合腹腔内热化疗(CRS-HIPEC)的患者术后疼痛管理和结局之间的关系。
在这项倾向匹配的回顾性队列研究中,我们进行了一项无同期对照组的前后研究。将接受 CRS-HIPEC 时实施 APS 的患者与历史对照(非 APS)患者的结局进行比较。主要目的是确定 APS 管理的患者在术后第 0-3 天期间的中位总阿片类药物消耗量是否降低。次要结局包括每个术后日(0-6 天)的阿片类药物消耗量、下床时间、固体摄入时间和住院时间。
排除后,共有 122 名患者,其中 APS 组和非 APS 组分别为 51 名和 71 名。在倾向匹配的两组之间,术后第 0-3 天的中位(四分位数)总阿片类药物消耗量分别为 27.5mg 静脉吗啡当量(MEQ)(7.6-106.3mg MEQ)和 144.0mg MEQ(68.9-238.3mg MEQ)。中位差值为 80.8mg MEQ(95%置信区间,46.1-124.0;P<0.0001)。APS 组的下床时间和固体饮食摄入时间均有统计学显著缩短。
实施 APS 后,CRS-HIPEC 患者的阿片类药物消耗量减少了>50%,下床时间和固体饮食摄入时间也缩短了。APS 的实施可能会改善 CRS-HIPEC 患者的结局。