Department of Diagnostic, Clinical and Public Health Medicine, University of Modena and Reggio Emilia, Modena, Italy
Yale University School of Medicine, New Haven, CT, USA.
Haematologica. 2018 Jul;103(7):1191-1197. doi: 10.3324/haematol.2017.186577. Epub 2018 Mar 29.
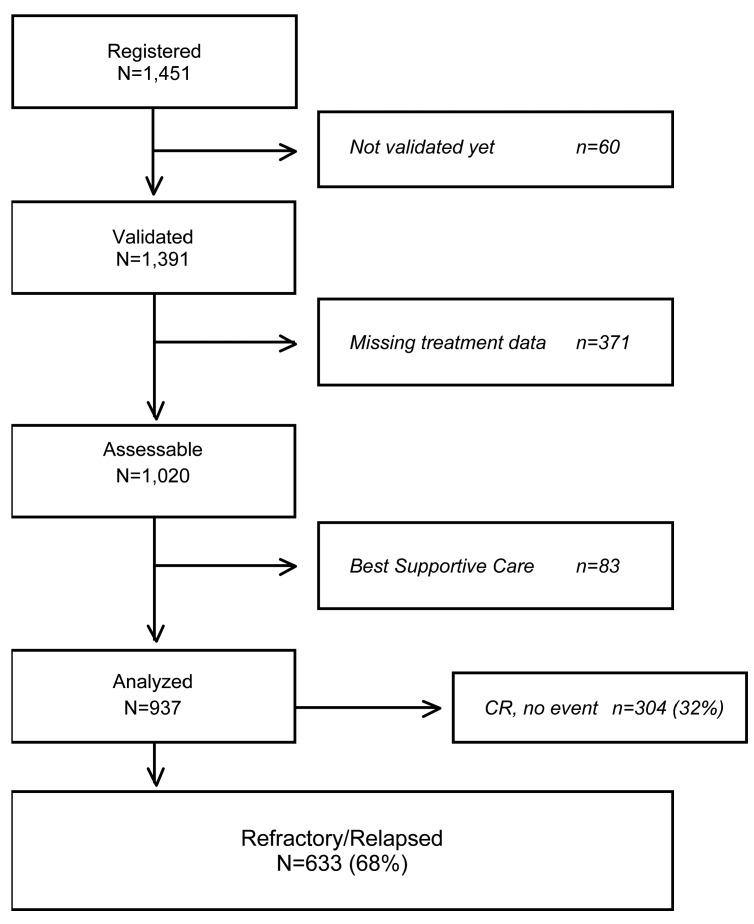
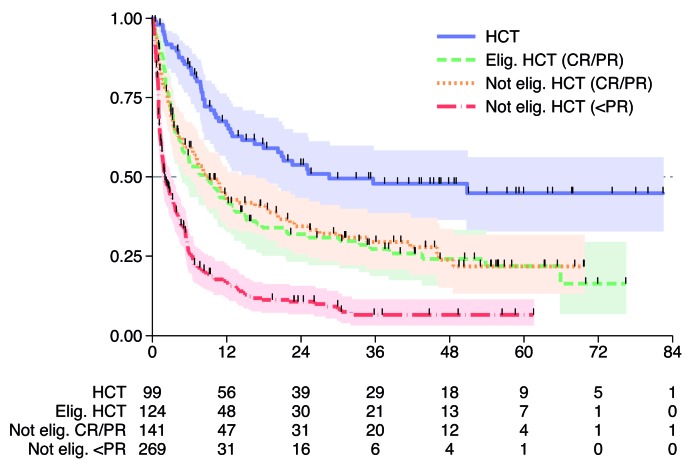
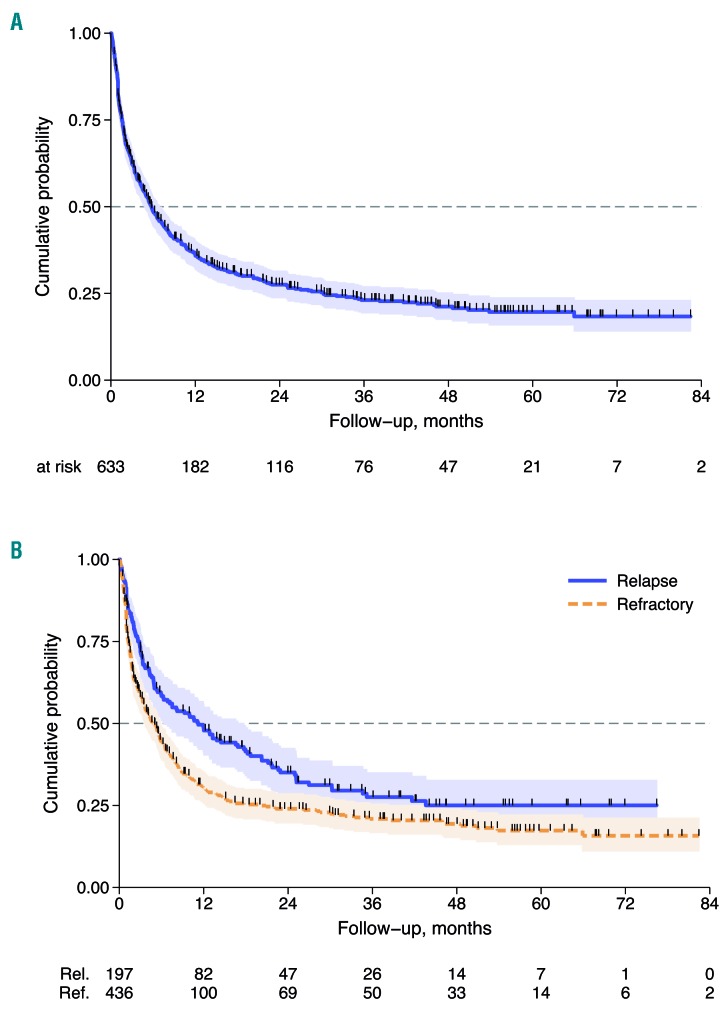
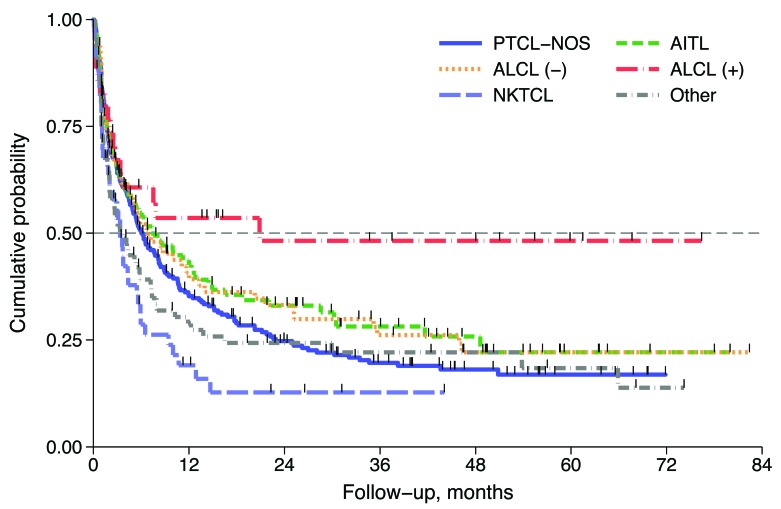
This analysis explored factors influencing survival of patients with primary refractory and relapsed peripheral T-cell lymphomas enrolled in the prospective International T-cell Project. We analyzed data from 1020 patients with newly diagnosed disease, enrolled between September 2006 and December 2015. Out of 937 patients who received first-line treatment, 436 (47%) were identified as refractory and 197 (21%) as relapsed. Median time from the end of treatment to relapse was 8 months (range 2-73). Overall, 75 patients (8%) were consolidated with bone marrow transplantation, including 12 refractory and 22 relapsed patients. After a median follow up of 38 months (range 1-96 months) from documentation of refractory/relapsed disease, 440 patients had died. The median overall survival (OS) was 5.8 months; 3-year overall survival rates were 21% and 28% for refractory and relapsed patients, respectively (<0.001). Patients receiving or not salvage bone marrow transplantation had a 3-year survival of 48% and 18%, respectively (<0.001). In a univariate Cox regression analysis, refractory disease was associated with a higher risk of death (HR=1.43, =0.001), whereas late relapse (>12 months, HR 0.57, =0.001) and salvage therapy with transplantation (HR=0.36, <0.001) were associated with a better OS. No difference was found in OS with respect to histology. This study accurately reflects outcomes for patients treated according to standards of care worldwide. Results confirm that peripheral T-cell lymphomas patients had dismal outcome after relapse or progression. Patients with chemotherapy sensitive disease who relapsed after more than 12 months might benefit from consolidation bone marrow transplantation.
本分析探讨了纳入国际 T 细胞项目前瞻性研究的原发性难治性和复发性外周 T 细胞淋巴瘤患者生存的影响因素。我们分析了 2006 年 9 月至 2015 年 12 月期间新诊断疾病的 1020 例患者的数据。在接受一线治疗的 937 例患者中,有 436 例(47%)被确定为难治性,197 例(21%)为复发性。从治疗结束到复发的中位时间为 8 个月(范围 2-73)。总体而言,75 例患者(8%)接受了骨髓移植巩固治疗,其中包括 12 例难治性和 22 例复发性患者。在难治性/复发性疾病记录后的中位随访 38 个月(范围 1-96 个月)后,有 440 例患者死亡。中位总生存期(OS)为 5.8 个月;难治性和复发性患者的 3 年总生存率分别为 21%和 28%(<0.001)。接受或未接受挽救性骨髓移植的患者 3 年生存率分别为 48%和 18%(<0.001)。在单变量 Cox 回归分析中,难治性疾病与死亡风险较高相关(HR=1.43,=0.001),而晚期复发(>12 个月,HR 0.57,=0.001)和挽救性移植治疗(HR=0.36,<0.001)与更好的 OS 相关。组织学与 OS 无差异。本研究准确反映了按照全球护理标准治疗的患者的结局。结果证实,外周 T 细胞淋巴瘤患者在复发或进展后预后不佳。化疗敏感疾病患者在 12 个月后复发可能受益于巩固性骨髓移植。