Universität Regensburg, Universitätsstraße 31, 93053, Regensburg, Germany.
Tumorzentrum Regensburg - Institut für Qualitätssicherung und Versorgungsforschung der Universität Regensburg, Am BioPark 9, 93053, Regensburg, Germany.
Surg Endosc. 2018 Oct;32(10):4138-4147. doi: 10.1007/s00464-018-6158-4. Epub 2018 Mar 30.
Over 20 years after the introduction of laparoscopic surgery for colon cancer, many surgeons still prefer the open approach. Whereas randomized controlled trials (RCTs) have proven the oncologic safety of laparoscopy, long-term data depicting daily clinical routine are scarce.
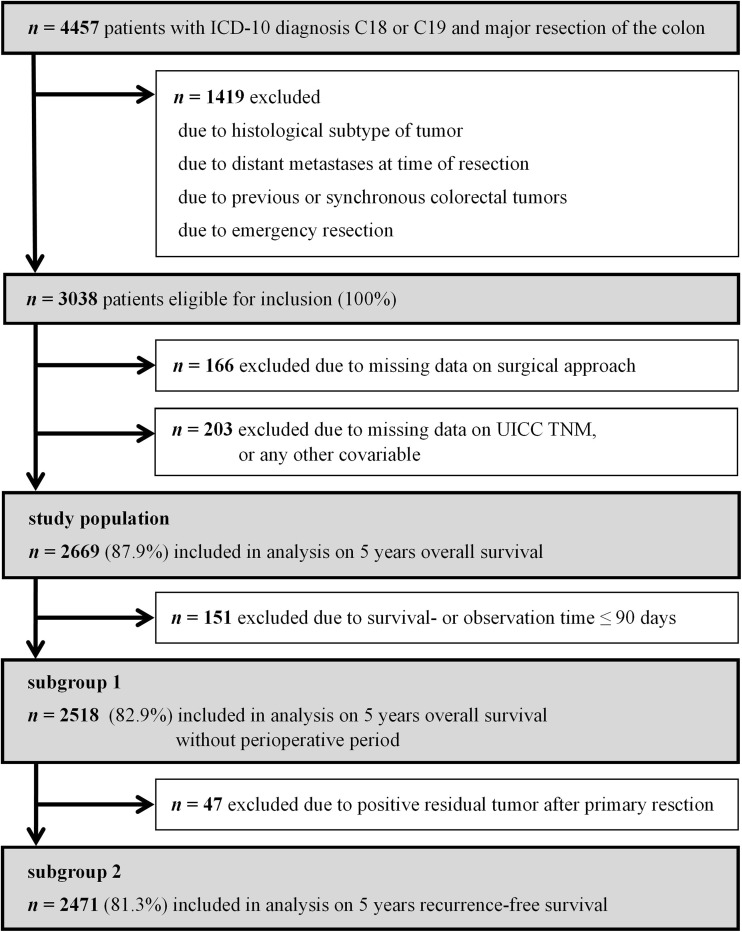
This population-based cohort study compares 5-year overall, relative, and recurrence-free survival rates after laparoscopic and open colon carcinoma surgery. Data derive from an independent German cancer registry encompassing all tumor patients within a political district of 1.1 million inhabitants. The final analysis included 2669 patients with major elective resection of primary non-metastatic colonic adenocarcinoma between January 1, 2004 and December 31, 2013. Survival rates were compared using Kaplan-Meier analyses, relative survival models, and multivariate Cox regression. Sensitivity analysis quantified selection bias.
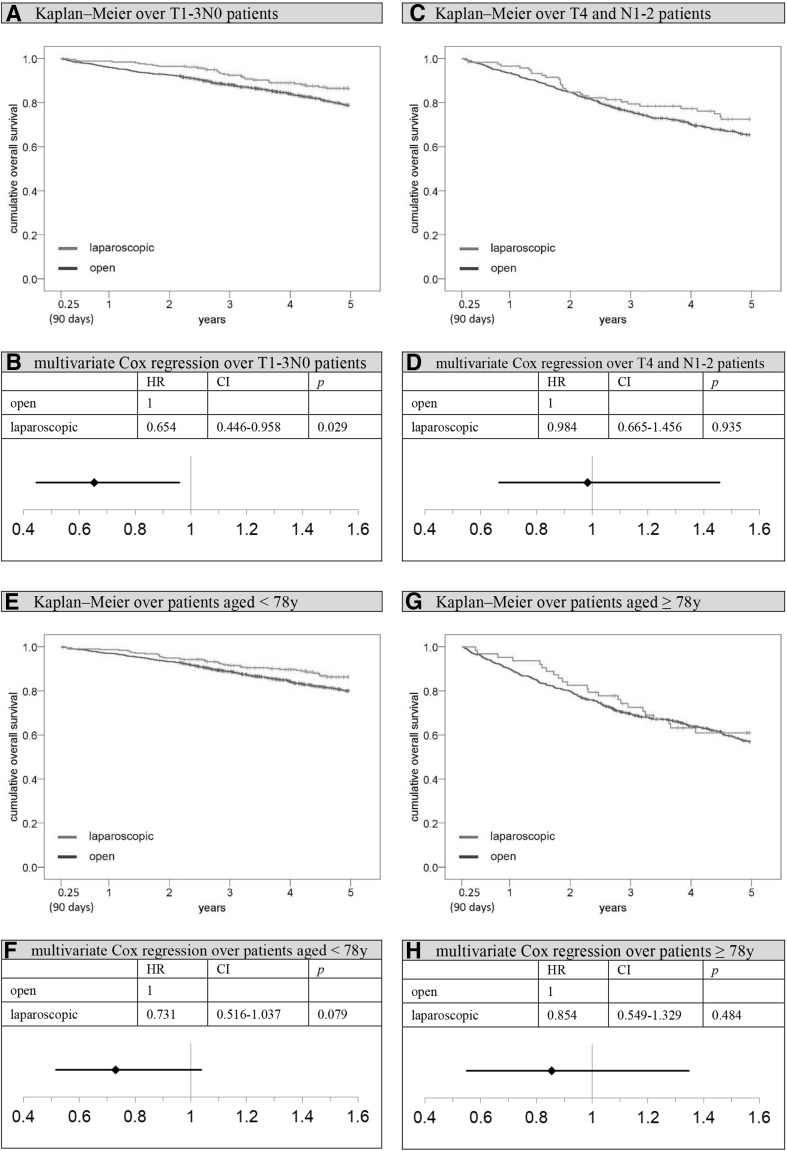
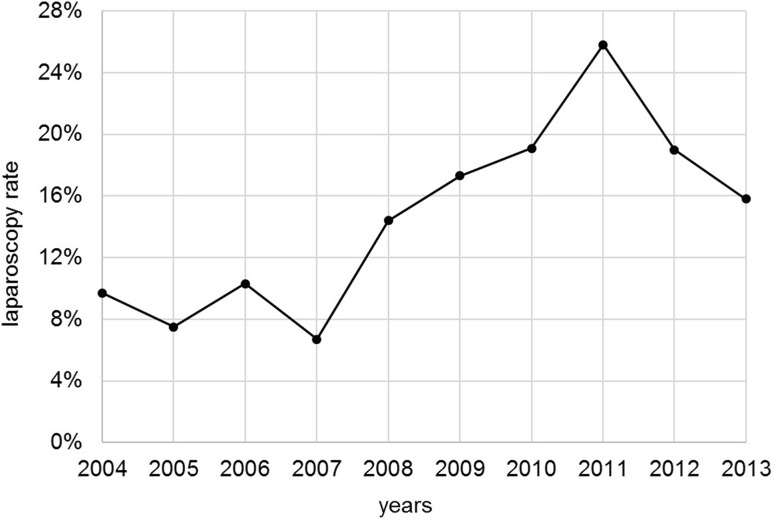
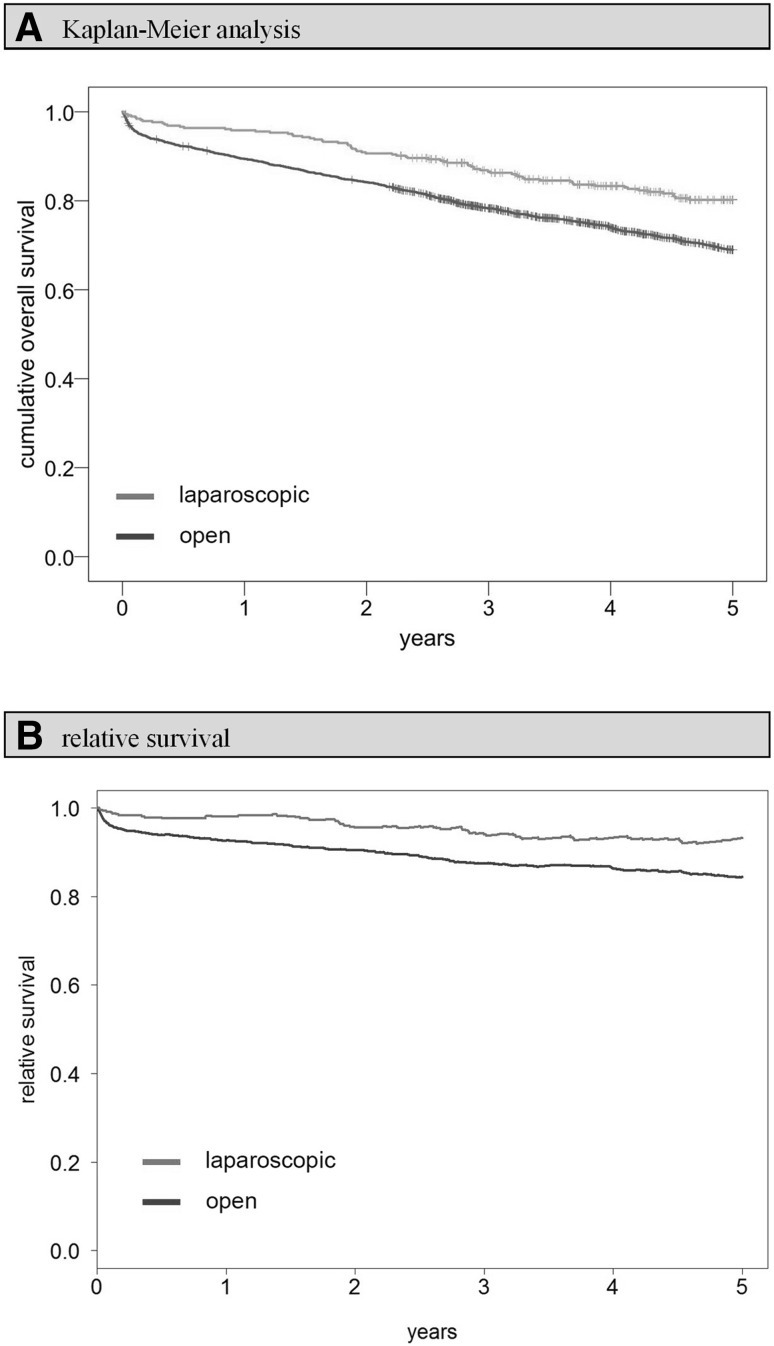
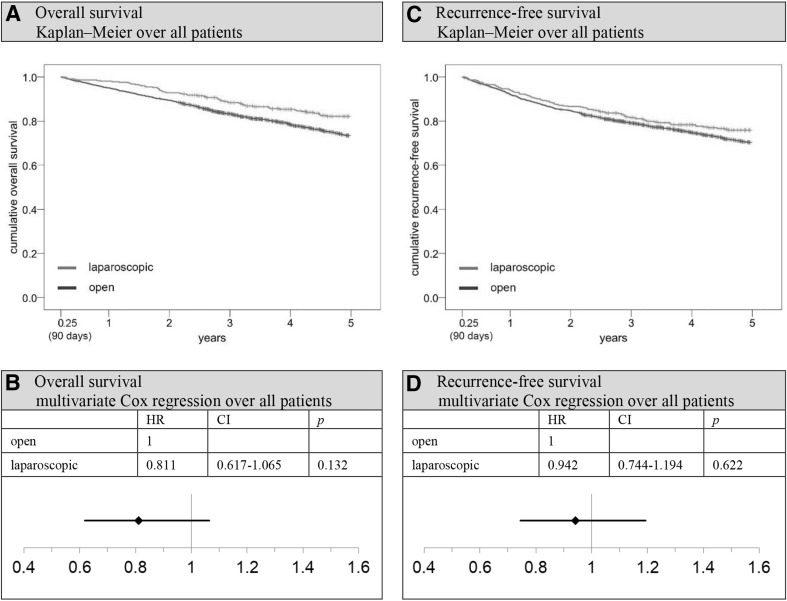
The proportion of laparoscopic procedures increased from 9.7 to 25.8% in 2011 and dropped again to 15.8% at the end of observation period. Laparoscopy patients were younger, had a lower tumor stage, and were more likely to receive postoperative chemotherapy. Overall, relative, and recurrence-free survival was significantly superior or equivalent in Kaplan-Meier analysis (5-year overall survival rate open vs. laparoscopic: 69.0 vs. 80.2%, p < 0.001). The superiority of laparoscopy mostly remained stable after adjusting for confounders, although significance was only reached in T1-3 patients without lymph node metastases (overall survival: hazard ratio (HR) 0.654; 95% confidence interval (CI) 0.446-0.958; p = 0.029).
Laparoscopy is a safe and promising alternative to the open approach in daily clinic practice. These favorable outcomes require future confirmation by high-quality studies outside the setting of RTCs.
腹腔镜手术应用于结肠癌已有 20 多年,但许多外科医生仍然更喜欢开放手术。虽然随机对照试验(RCT)已经证明了腹腔镜手术的肿瘤安全性,但缺乏描述日常临床实践的长期数据。
本基于人群的队列研究比较了腹腔镜和开腹结肠癌手术后 5 年的总生存率、相对生存率和无复发生存率。数据来自一个独立的德国癌症登记处,涵盖了一个拥有 110 万居民的行政区内的所有肿瘤患者。最终分析包括 2004 年 1 月 1 日至 2013 年 12 月 31 日期间接受主要择期原发性非转移性结肠腺癌切除术的 2669 例患者。使用 Kaplan-Meier 分析、相对生存模型和多变量 Cox 回归比较生存率。敏感性分析量化了选择偏倚。
腹腔镜手术的比例从 2011 年的 9.7%增加到 25.8%,在观察期结束时又下降到 15.8%。腹腔镜手术患者年龄较小,肿瘤分期较低,术后更有可能接受化疗。在 Kaplan-Meier 分析中,总生存率、相对生存率和无复发生存率显著提高或相当(5 年总生存率开腹与腹腔镜:69.0%与 80.2%,p<0.001)。调整混杂因素后,腹腔镜的优势基本保持稳定,尽管在无淋巴结转移的 T1-3 患者中具有统计学意义(总生存:风险比(HR)0.654;95%置信区间(CI)0.446-0.958;p=0.029)。
在日常临床实践中,腹腔镜是开放手术的一种安全且有前途的替代方法。这些有利的结果需要未来在 RCT 之外的高质量研究中得到证实。