University of Texas Southwestern Medical Center/Children's Health, Dallas, TX, USA.
Dana-Farber/Boston Children's Cancer and Blood Disorders Center and Harvard Medical School, Boston, MA, USA.
Lancet Oncol. 2018 May;19(5):705-714. doi: 10.1016/S1470-2045(18)30119-0. Epub 2018 Mar 29.
Gene fusions involving NTRK1, NTRK2, or NTRK3 (TRK fusions) are found in a broad range of paediatric and adult malignancies. Larotrectinib, a highly selective small-molecule inhibitor of the TRK kinases, had shown activity in preclinical models and in adults with tumours harbouring TRK fusions. This study aimed to assess the safety of larotrectinib in paediatric patients.
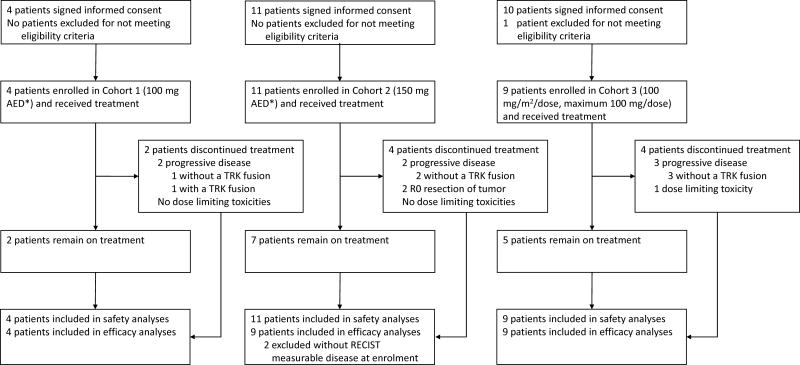
This multicentre, open-label, phase 1/2 study was done at eight sites in the USA and enrolled infants, children, and adolescents aged 1 month to 21 years with locally advanced or metastatic solid tumours or CNS tumours that had relapsed, progressed, or were non-responsive to available therapies regardless of TRK fusion status; had a Karnofsky (≥16 years of age) or Lansky (<16 years of age) performance status score of 50 or more, adequate organ function, and full recovery from the acute toxic effects of all previous anticancer therapy. Following a protocol amendment on Sept 12, 2016, patients with locally advanced infantile fibrosarcoma who would require disfiguring surgery to achieve a complete surgical resection were also eligible. Patients were enrolled to three dose cohorts according to a rolling six design. Larotrectinib was administered orally (capsule or liquid formulation), twice daily, on a continuous 28-day schedule, in increasing doses adjusted for age and bodyweight. The primary endpoint of the phase 1 dose escalation component was the safety of larotrectinib, including dose-limiting toxicity. All patients who received at least one dose of larotrectinib were included in the safety analyses. Reported here are results of the phase 1 dose escalation cohort. Phase 1 follow-up and phase 2 are ongoing. This trial is registered with ClinicalTrials.gov, number NCT02637687.
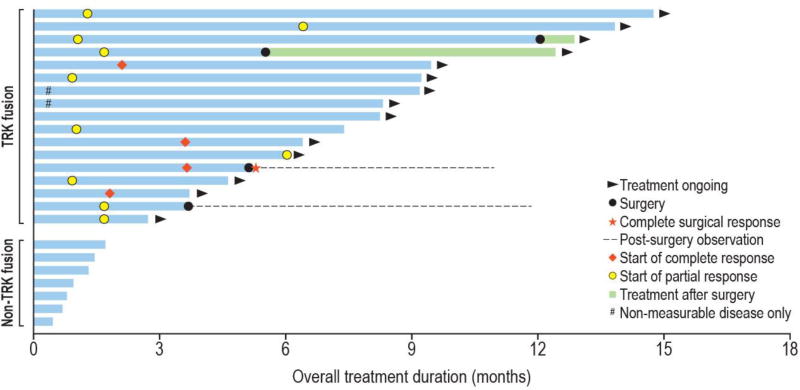
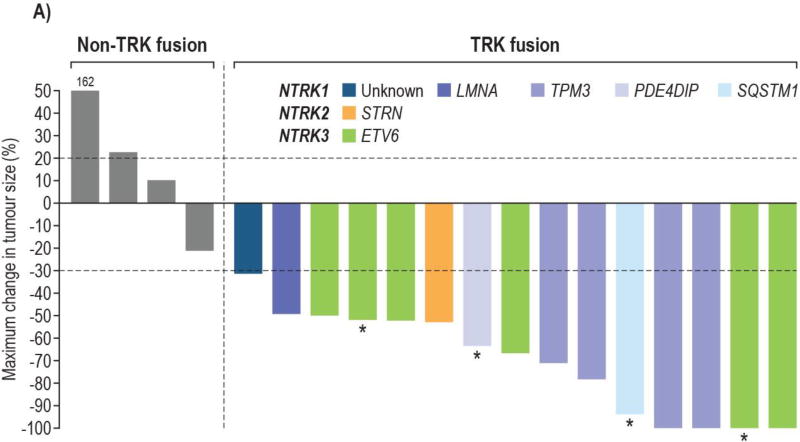
Between Dec 21, 2015, and April 13, 2017, 24 patients (n=17 with tumours harbouring TRK fusions, n=7 without a documented TRK fusion) with a median age of 4·5 years (IQR 1·3-13·3) were enrolled to three dose cohorts: cohorts 1 and 2 were assigned doses on the basis of both age and bodyweight predicted by use of SimCyp modelling to achieve an area under the curve equivalent to the adult doses of 100 mg twice daily (cohort 1) and 150 mg twice daily (cohort 2); and cohort 3 was assigned to receive a dose of 100 mg/m twice daily (maximum 100 mg per dose), regardless of age, equating to a maximum of 173% of the recommended adult phase 2 dose. Among enrolled patients harbouring TRK fusion-positive cancers, eight (47%) had infantile fibrosarcoma, seven (41%) had other soft tissue sarcomas, and two (12%) had papillary thyroid cancer. Adverse events were predominantly grade 1 or 2 (occurring in 21 [88%] of 24 patients); the most common larotrectinib-related adverse events of all grades were increased alanine and aspartate aminotransferase (ten [42%] of 24 each), leucopenia (five [21%] of 24), decreased neutrophil count (five [21%] of 24), and vomiting (five [21%] of 24). Grade 3 alanine aminotransferase elevation was the only dose-limiting toxicity and occurred in one patient without a TRK fusion and with progressive disease. No grade 4 or 5 treatment-related adverse events were observed. Two larotrectinib-related serious adverse events were observed: grade 3 nausea and grade 3 ejection fraction decrease during the 28-day follow-up after discontinuing larotrectinib and while on anthracyclines. The maximum tolerated dose was not reached, and 100 mg/m (maximum of 100 mg per dose) was established as the recommended phase 2 dose. 14 (93%) of 15 patients with TRK fusion-positive cancers achieved an objective response as per Response Evaluation Criteria In Solid Tumors version 1.1; the remaining patient had tumour regression that did not meet the criteria for objective response. None of the seven patients with TRK fusion-negative cancers had an objective response.
The TRK inhibitor larotrectinib was well tolerated in paediatric patients and showed encouraging antitumour activity in all patients with TRK fusion-positive tumours. The recommended phase 2 dose was defined as 100mg/m (maximum 100 mg per dose) for infants, children, and adolescents, regardless of age.
Loxo Oncology Inc.
NTRK1、NTRK2 或 NTRK3 基因融合(TRK 融合)存在于广泛的儿科和成人恶性肿瘤中。拉罗替尼是一种高度选择性的 TRK 激酶小分子抑制剂,在临床前模型和携带 TRK 融合的肿瘤的成人中显示出活性。本研究旨在评估拉罗替尼在儿科患者中的安全性。
这项多中心、开放标签、1/2 期研究在美国的 8 个地点进行,招募了 1 个月至 21 岁的局部晚期或转移性实体瘤或中枢神经系统肿瘤的婴儿、儿童和青少年患者,这些患者既往接受过治疗但疾病复发、进展或对现有治疗方案无反应,无论 TRK 融合状态如何;卡氏(Karnofsky)评分(年龄≥ 16 岁)或 Lansky(Lansky)评分(年龄<16 岁)为 50 或更高,器官功能良好,且所有既往抗癌治疗的急性毒性反应完全恢复。2016 年 9 月 12 日,在一项方案修正案后,也有符合条件的局部晚期婴儿纤维肉瘤患者,他们需要进行毁容手术才能实现完全手术切除。根据滚动 6 设计,患者被分为三个剂量组。拉罗替尼口服(胶囊或液体制剂),每日两次,连续 28 天,剂量根据年龄和体重进行调整。1 期剂量递增部分的主要终点是拉罗替尼的安全性,包括剂量限制性毒性。所有接受至少一剂拉罗替尼治疗的患者均纳入安全性分析。在此报告 1 期剂量递增队列的结果。1 期随访和 2 期正在进行中。该试验在 ClinicalTrials.gov 注册,编号为 NCT02637687。
2015 年 12 月 21 日至 2017 年 4 月 13 日,24 例患者(n=17 例肿瘤携带 TRK 融合,n=7 例无记录的 TRK 融合)纳入 3 个剂量组:第 1 组和第 2 组根据使用 SimCyp 模型预测的年龄和体重进行剂量分配,以达到与成人每日 100 mg 两次、150 mg 两次等效的 AUC(第 1 组)和 150 mg 两次(第 2 组);第 3 组分配接受 100 mg/m 两次(最大剂量为 100 mg/次),无论年龄如何,相当于推荐的成人 2 期剂量的 173%。在入组的携带 TRK 融合阳性癌症的患者中,8 例(47%)患有婴儿纤维肉瘤,7 例(41%)患有其他软组织肉瘤,2 例(12%)患有甲状腺乳头状癌。不良事件主要为 1 级或 2 级(24 例患者中的 21 例[88%]);所有级别中最常见的拉罗替尼相关不良事件为丙氨酸转氨酶和天冬氨酸转氨酶升高(24 例患者各 10 例[42%])、白细胞减少(24 例患者各 5 例[21%])、中性粒细胞计数减少(24 例患者各 5 例[21%])和呕吐(24 例患者各 5 例[21%])。丙氨酸氨基转移酶升高 3 级是唯一的剂量限制毒性,发生在一名无 TRK 融合且疾病进展的患者中。未观察到 4 级或 5 级与治疗相关的不良事件。观察到 2 例与拉罗替尼相关的严重不良事件:在停止拉罗替尼并使用蒽环类药物后 28 天的随访期间观察到 3 级恶心和 3 级射血分数降低。未达到最大耐受剂量,确定 100 mg/m(最大剂量为 100 mg/次)为推荐的 2 期剂量。15 例携带 TRK 融合阳性癌症的患者中,14 例(93%)根据实体瘤反应评估标准 1.1 达到客观缓解;其余 1 例患者的肿瘤消退不符合客观缓解的标准。7 例携带 TRK 融合阴性癌症的患者均未达到客观缓解。
TRK 抑制剂拉罗替尼在儿科患者中耐受性良好,在所有携带 TRK 融合阳性肿瘤的患者中显示出令人鼓舞的抗肿瘤活性。定义为 100mg/m(最大剂量为 100mg/次)的推荐 2 期剂量适用于婴儿、儿童和青少年,无论年龄如何。
Loxo Oncology Inc.