Goirand Maxime, Breton Sylvain, Chevallier Frédéric, Duong Ngoc-Phoi, Uettwiller Florence, Melki Isabelle, Mouy Richard, Wouters Carine, Bader-Meunier Brigitte, Job-Deslandre Chantal, Quartier Pierre
Pediatric Immunology, Hematology, and Rheumatology Unit, Centre de Référence pour les Rhumatismes Inflammatoires et les Maladies Auto-Immunes Systémique Rare de l'Enfant (RAISE) ; Necker-Enfants Malades Hospital, Assistance Publique Hôpitaux de Paris, 149, rue de Sèvres, 75743 Cedex15, Paris, France.
Paris Descartes University, 12 rue de l'Ecole de Médicine, 75006, Paris, France.
Pediatr Rheumatol Online J. 2018 Apr 2;16(1):21. doi: 10.1186/s12969-018-0238-9.
Childhood-onset spondyloarthropathies usually start with enthesitis and peripheral arthritis. However, axial disease may develop afterward. Patients are most often classified, following revised (Edmonton 2011) ILAR criteria, as enthesitis-related arthritis, psoriatic arthritis, or unclassified juvenile idiopathic arthritis, particularly in cases of psoriasis in the patient or a first-degree relative. In adults, peripheral spondyloarthritis is classified by ASAS criteria.
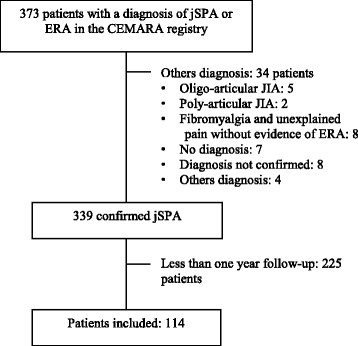
We retrospectively studied patients with childhood-onset spondyloarthropathies followed for more than one year in our referral centre. We did not exclude patients with a personal or familial history of psoriasis.
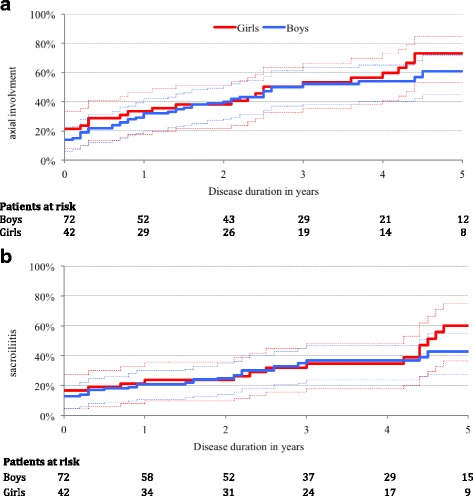
We included 114 patients followed between January 2008 and December 2015 for a median of 2.5 years (IQR = 2.3). Sixty-nine per-cent of patients fulfilled the revised ILAR classification criteria for enthesitis-related arthritis, and 92% the ASAS criteria for peripheral spondyolarthritis (p < 0.001). Axial disease and sacroiliitis were rare at disease onset. However, they appeared during follow-up in 63% and 47% of cases respectively, after a median disease duration of 2.6 (IC 95% [2.2-4.4]) and 5.3 years (IC 95% [4.1-7.7]), respectively. Multivariable analysis showed that familial history of spondyloarthritis was associated with the presence of sacroiliitis and active disease at the latest follow-up (OR = 3.61 [1.5-8.7], p < 0.01 and 2.98 [1.2-7.3], p = 0.02, respectively).
Axial involvement developed in most patients within five years. Revised Edmonton criteria were less sensitive than ASAS criteria to classify patients as having childhood-onset spondyloarthropathies. The main risk factor for both sacroiliitis and persistent active disease was a familial history of spondyloarthritis.
儿童期起病的脊柱关节炎通常始于附着点炎和外周关节炎。然而,之后可能会出现中轴疾病。根据修订后的(2011年埃德蒙顿)国际风湿病联盟(ILAR)标准,患者最常被分类为附着点炎相关关节炎、银屑病关节炎或未分类的幼年特发性关节炎,尤其是患者或一级亲属中有银屑病的情况。在成人中,外周型脊柱关节炎根据脊柱关节炎国际学会(ASAS)标准进行分类。
我们回顾性研究了在我们的转诊中心随访超过一年的儿童期起病的脊柱关节炎患者。我们没有排除有个人或家族银屑病病史的患者。
我们纳入了2008年1月至2015年12月期间随访的114例患者,中位随访时间为2.5年(四分位间距=2.3)。69%的患者符合修订后的ILAR附着点炎相关关节炎分类标准,92%符合ASAS外周型脊柱关节炎标准(p<0.001)。疾病初发时中轴疾病和骶髂关节炎很少见。然而,在随访期间,分别有63%和47%的病例出现了中轴疾病和骶髂关节炎,中位病程分别为2.6年(95%置信区间[2.2 - 4.4])和5.3年(95%置信区间[4.1 - 7.7])。多变量分析显示,脊柱关节炎家族史与最新随访时骶髂关节炎的存在及疾病活动相关(比值比分别为3.61[1.5 - 8.7],p<0.01和2.98[1.2 - 7.3],p = 0.02)。
大多数患者在五年内出现中轴受累。修订后的埃德蒙顿标准在将患者分类为儿童期起病的脊柱关节炎方面不如ASAS标准敏感。骶髂关节炎和持续性疾病活动的主要危险因素是脊柱关节炎家族史。