Departments of Surgery.
Department of Gastroenterological Surgery, Cancer Institute Hospital, Japanese Foundation for Cancer Research, Tokyo.
Am J Surg Pathol. 2018 Jun;42(6):705-714. doi: 10.1097/PAS.0000000000001059.
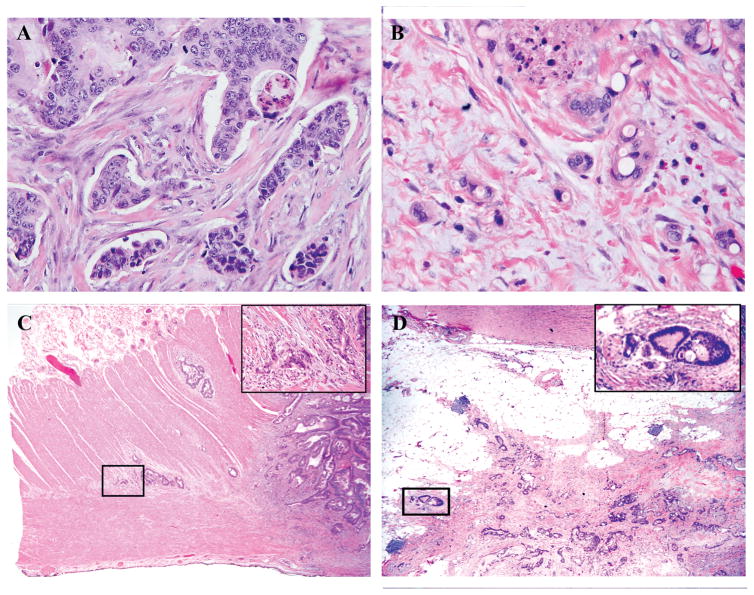
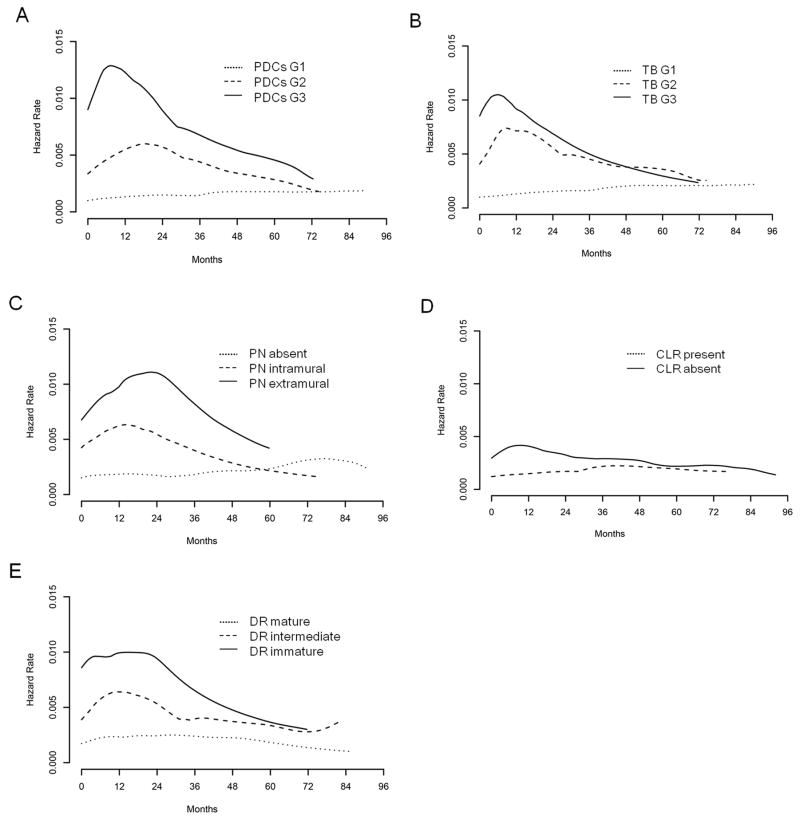
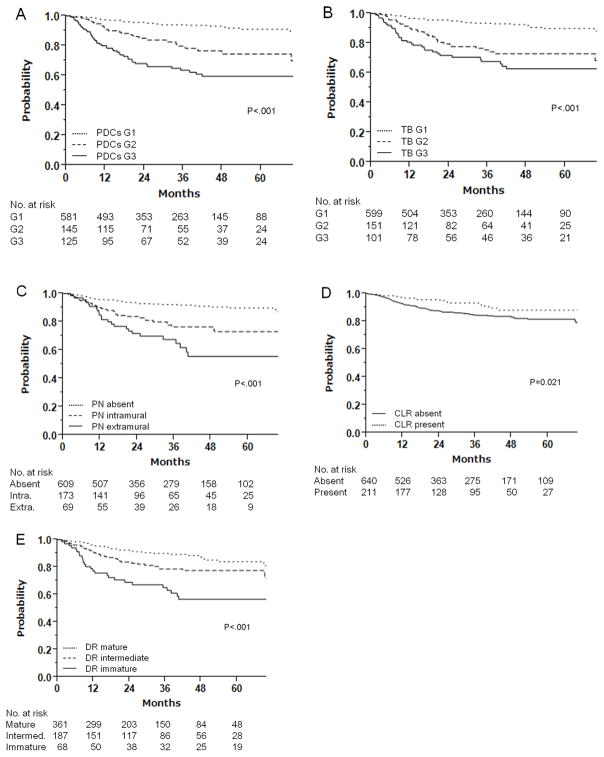
This study aimed to compare common histologic markers at the invasive front of colon adenocarcinoma in terms of prognostic accuracy and interobserver agreement. Consecutive patients who underwent curative resection for stages I to III colon adenocarcinoma at a single institution in 2007 to 2014 were identified. Poorly differentiated clusters (PDCs), tumor budding, perineural invasion, desmoplastic reaction, and Crohn-like lymphoid reaction at the invasive front, as well as the World Health Organization (WHO) grade of the entire tumor, were analyzed. Prognostic accuracies for recurrence-free survival (RFS) were compared, and interobserver agreement among 3 pathologists was assessed. The study cohort consisted of 851 patients. Although all the histologic markers except WHO grade were significantly associated with RFS (PDCs, tumor budding, perineural invasion, and desmoplastic reaction: P<0.001; Crohn-like lymphoid reaction: P=0.021), PDCs (grade 1 [G1]: n=581; G2: n=145; G3: n=125) showed the largest separation of 3-year RFS in the full cohort (G1: 94.1%; G3: 63.7%; hazard ratio [HR], 6.39; 95% confidence interval [CI], 4.11-9.95; P<0.001), stage II patients (G1: 94.0%; G3: 67.3%; HR, 4.15; 95% CI, 1.96-8.82; P<0.001), and stage III patients (G1: 89.0%; G3: 59.4%; HR, 4.50; 95% CI, 2.41-8.41; P<0.001). PDCs had the highest prognostic accuracy for RFS with the concordance probability estimate of 0.642, whereas WHO grade had the lowest. Interobserver agreement was the highest for PDCs, with a weighted kappa of 0.824. The risk of recurrence over time peaked earlier for worse PDCs grade. Our findings indicate that PDCs are the best invasive-front histologic marker in terms of prognostic accuracy and interobserver agreement. PDCs may replace WHO grade as a prognostic indicator.
这项研究旨在比较结肠癌浸润前沿的常见组织学标志物在预测准确性和观察者间一致性方面的差异。在 2007 年至 2014 年期间,我们从一家机构接受根治性切除术治疗 I 至 III 期结肠癌的连续患者中确定了这一点。在浸润前沿分析了分化不良簇(PDCs)、肿瘤芽殖、神经周围侵犯、纤维反应和克罗恩样淋巴反应,以及整个肿瘤的世界卫生组织(WHO)分级。比较了无复发生存(RFS)的预测准确性,并评估了 3 位病理学家之间的观察者间一致性。研究队列包括 851 名患者。虽然所有组织学标志物(除了 WHO 分级外)均与 RFS 显著相关(PDCs、肿瘤芽殖、神经周围侵犯和纤维反应:P<0.001;克罗恩样淋巴反应:P=0.021),但 PDCs(分级 1 [G1]:n=581;G2:n=145;G3:n=125)在整个队列中显示出最大的 3 年 RFS 分离(G1:94.1%;G3:63.7%;危险比[HR],6.39;95%置信区间[CI],4.11-9.95;P<0.001),在 II 期患者(G1:94.0%;G3:67.3%;HR,4.15;95%CI,1.96-8.82;P<0.001)和 III 期患者(G1:89.0%;G3:59.4%;HR,4.50;95%CI,2.41-8.41;P<0.001)。PDCs 对 RFS 的预测准确性最高,一致性概率估计值为 0.642,而 WHO 分级最低。PDCs 的观察者间一致性最高,加权kappa 值为 0.824。随着时间的推移,PDCs 分级越差,复发的风险越高。我们的研究结果表明,在预测准确性和观察者间一致性方面,PDCs 是最好的浸润前沿组织学标志物。PDCs 可能取代 WHO 分级作为预后指标。