Lian Ingrid Alsos, Åsberg Arne
Department of Clinical Chemistry, St.Olavs hospital, Trondheim, Norway.
BMJ Open. 2018 Apr 7;8(4):e017703. doi: 10.1136/bmjopen-2017-017703.
Albumin-adjusted total calcium is often used as a surrogate marker for free calcium to evaluate hypocalcaemia or hypercalcaemia. Many adjustment formulas based on simple linear regression models have been published, and continue to be used in spite of questionable diagnostic accuracy. In the hope of finding a more pure albumin effect on total calcium, we used multiple linear regression models to adjust for other relevant variables. The regression coefficients of albumin were used to construct local adjustment formulas, and we tested whether the diagnostic accuracy was improved compared with previously published formulas and unadjusted calcium.
A retrospective hospital laboratory data study.
The local hospital laboratory data system.
Norway, 2006-2015.
6549 patients above 2 years of age, where free calcium standardised at pH 7.40, total calcium, creatinine, albumin and phosphate had been analysed in a single blood draw, including hospitalised patients and patients from outpatient clinics and general practice.
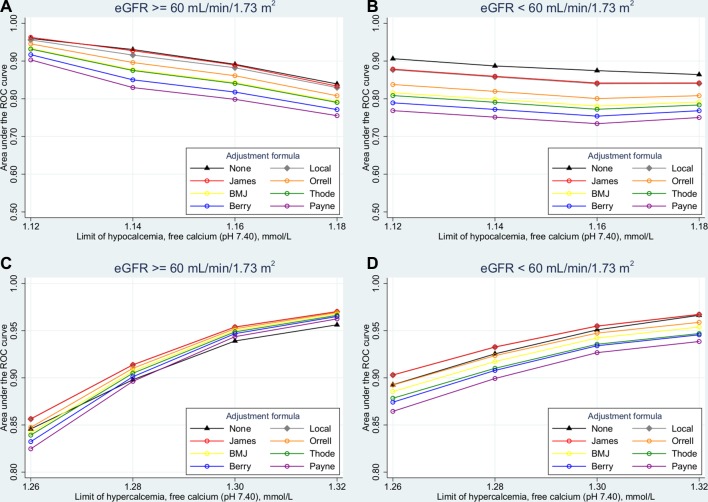
Diagnostic accuracy by Harrell's c and receiver operating characteristic curve analysis, using free calcium standardised at pH 7.40 as a gold standard, in subgroups with estimated glomerular filtration rate (eGFR) ≥60 or <60 mL/min/1.73 m.
In the subgroup with eGFR <60 mL/min/1.73 m, the Harrell's c of unadjusted total calcium (0.801) was significantly larger than those of the local formulas (0.790, p=0.002) and the best formula taken from literature (0.791, p=0.004). In the subgroup with eGFR ≥60 mL/min/1.73 m, no significant differences were found between these three formulas.
Our study shows that the diagnostic accuracy of total calcium is superior to several commonly used adjustment formulas, and we suggest that the use of such formulas should be abandoned in clinical practice. If the clinician does not trust total calcium to reflect the calcium status of the patient, free calcium should be measured.
校正白蛋白后的总钙常被用作游离钙的替代标志物,以评估低钙血症或高钙血症。许多基于简单线性回归模型的校正公式已发表,尽管诊断准确性存疑,但仍在继续使用。为了找到白蛋白对总钙更纯粹的影响,我们使用多元线性回归模型对其他相关变量进行校正。白蛋白的回归系数用于构建局部校正公式,我们测试了与先前发表的公式和未校正的钙相比,诊断准确性是否有所提高。
一项回顾性医院实验室数据研究。
当地医院实验室数据系统。
挪威,2006 - 2015年。
6549名2岁以上患者,在一次血液检测中分析了pH值为7.40时的游离钙、总钙、肌酐、白蛋白和磷酸盐,包括住院患者以及门诊和全科医疗的患者。
采用Harrell's c和受试者工作特征曲线分析诊断准确性,以pH值为7.40时标准化的游离钙作为金标准,在估计肾小球滤过率(eGFR)≥60或<60 mL/min/1.73 m²的亚组中进行分析。
在eGFR <60 mL/min/1.73 m²的亚组中,未校正的总钙的Harrell's c(0.801)显著大于局部公式(0.790,p = 0.002)和文献中最佳公式(0.791,p = 0.004)。在eGFR≥60 mL/min/1.73 m²的亚组中,这三个公式之间未发现显著差异。
我们的研究表明,总钙的诊断准确性优于几种常用的校正公式,我们建议在临床实践中应放弃使用此类公式。如果临床医生不信任总钙能反映患者的钙状态,则应检测游离钙。