Güneş Selçuk, Orhan Kadir Serkan, Başaran Bora, Çelik Mehmet, Kıyak Erkan
Istanbul University, Faculty of Medicine, Department of Otolaryngology Head and Neck Surgery, Istanbul, Turkey; Bakırköy Dr Sadi Konuk Research and Teaching Hospital, Department of Otolaryngology Head and Neck Surgery, Istanbul, Turkey.
Istanbul University, Faculty of Medicine, Department of Otolaryngology Head and Neck Surgery, Istanbul, Turkey.
Braz J Otorhinolaryngol. 2019 May-Jun;85(3):344-350. doi: 10.1016/j.bjorl.2018.02.007. Epub 2018 Mar 24.
Laryngeal cancer is the most common cancer of the upper respiratory tract. The main methods of treatment included surgery (partial laryngectomy and total laryngectomy) and radiation therapy. Laryngeal dysfunction is seen after both treatment modalities.
The aim of the study is to compare postoperative functional results of the standard supracricoid partial laryngectomy technique and a modified supracricoid partial laryngectomy technique using the sternohyoid muscle.
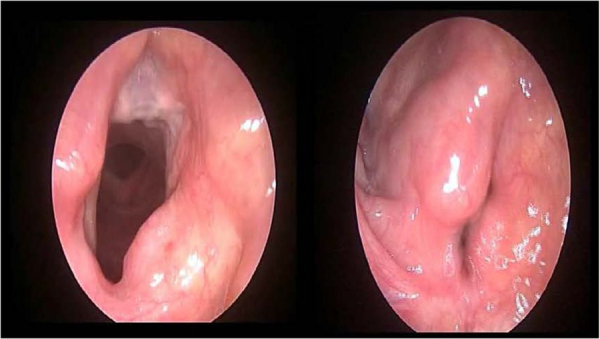
In total, 29 male patients (average years 58.20±9.00 years; range 41-79 years) with laryngeal squamous cell carcinoma who underwent supra cricoid partial laryngectomy were included. The patients were divided into two groups in terms of the surgical techniques. In Group A, all patients underwent standard supracricoid partial laryngectomy technique between January 2007 and November 2011. In Group B, all patients underwent modified supracricoid partial laryngectomy between August 2010 and November 2011. Fiberoptic endoscopic evaluation of swallowing test, short version of the voice handicap index scores, and the MD Anderson dysphagia inventory, the time of oral feeding and the decanulation of the patients after surgery of each groups were compared.
The mean maximum phonation time was 8.68±4.21s in Group A and 15.24±6.16s in Group B (p>0.05). The S/Z (s/s) ratio was 1.23±0.35 in Group A and 1.08±0.26 in Group B (p>0.05); the voice handicap index averages were 9.86±4.77 in Group A and 12.42±12.54 in Group B (p>0.05); the fiberoptic endoscopic evaluation of swallowing test averages were calculated as 12.73±3.08 in Group A and 13.64±1.49 in Group B (p>0.05). In the MD Anderson dysphagia inventory, evaluation of swallowing, the emotional, physical, and functional scores were 29.21±4.11, 32.21±6.85, and 20.14±2.17 in the Group B, and 29.20±2.54, 32.4±4.79, and 19±1.92 in Group A, respectively.
Although there is no statistical difference in functional outcome comparisons, if rules are adhered to in preoperative patient selection, modified supracricoid partial laryngectomy can be applied safely and meaningful gains can be achieved in functional outcomes.
喉癌是上呼吸道最常见的癌症。主要治疗方法包括手术(部分喉切除术和全喉切除术)和放射治疗。两种治疗方式后均会出现喉功能障碍。
本研究旨在比较标准环状软骨上部分喉切除术技术与使用胸骨舌骨肌的改良环状软骨上部分喉切除术技术的术后功能结果。
总共纳入29例接受环状软骨上部分喉切除术的男性喉鳞状细胞癌患者(平均年龄58.20±9.00岁;范围41 - 79岁)。根据手术技术将患者分为两组。A组,所有患者在2007年1月至2011年11月期间接受标准环状软骨上部分喉切除术技术。B组,所有患者在2010年8月至2011年11月期间接受改良环状软骨上部分喉切除术。比较两组患者术后吞咽试验的纤维内镜评估、嗓音障碍指数简表评分、MD安德森吞咽量表、经口进食时间和拔管时间。
A组平均最大发声时间为8.68±4.21秒,B组为15.24±6.16秒(p>0.05)。A组S/Z(s/s)比值为1.23±0.35,B组为1.08±0.26(p>0.05);A组嗓音障碍指数平均值为9.86±4.77,B组为12.42±12.54(p>0.05);A组吞咽试验的纤维内镜评估平均值计算为12.73±3.08,B组为13.64±1.49(p>0.05)。在MD安德森吞咽量表中,B组吞咽、情感、身体和功能评分分别为29.21±4.11、32.21±6.85和20.14±2.17,A组分别为29.20±2.54、32.4±4.79和19±1.92。
尽管功能结果比较无统计学差异,但如果在术前患者选择中遵循相关规则,改良环状软骨上部分喉切除术可安全应用,并能在功能结果上取得有意义的改善。