Kwon Hye-Mee, Moon Young-Jin, Jung Kyeo-Woon, Jeong Hye-Won, Park Yong-Seok, Jun In-Gu, Song Jun-Gol, Hwang Gyu-Sam
Department of Anesthesiology and Pain Medicine, Laboratory for Cardiovascular Dynamics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea.
Anesthesiology and Pain Medicine, Laboratory for Cardiovascular Dynamics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea.
Ann Transplant. 2018 Apr 10;23:236-245. doi: 10.12659/AOT.908329.
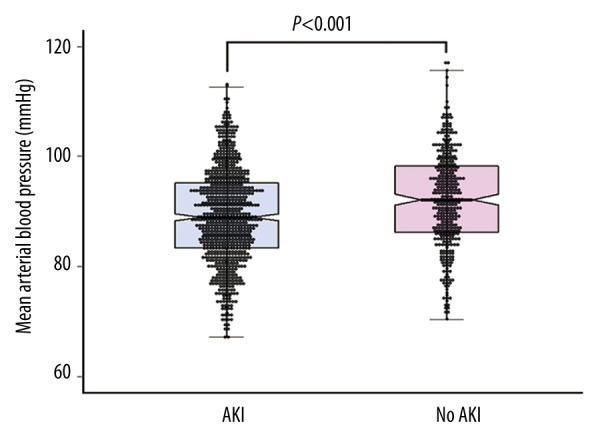
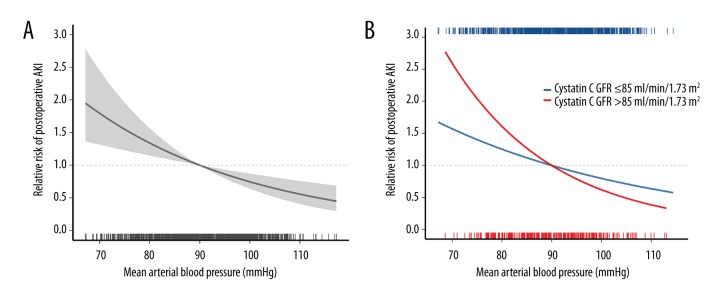
BACKGROUND As end-stage liver disease progresses, renal blood flow linearly correlates with mean arterial blood pressure (MBP) due to impaired autoregulation. We investigated whether the lower degree of postoperative MBP would predict the occurrence of postoperative acute kidney injury (AKI) after liver transplantation. MATERIAL AND METHODS This retrospective study enrolled 1,136 recipients with normal preoperative kidney function. Patients were categorized into two groups according to the averaged postoperative MBP: <90 mmHg (MBPbelow90) and ≥90 mmHg (MBPover90). The primary endpoint was occurrence of postoperative AKI, defined by the creatinine criteria of the Kidney Disease Improving Global Outcomes. The logistic regression model with inverse probability treatment weighting (IPTW) of propensity score was used to compare the risk of postoperative AKI between two groups. RESULTS MBPbelow90 group (83.0±5.1 mmHg) showed higher prevalence and risk of postoperative AKI (74.2% versus 62.6%, p<0.001; IPTW-OR 1.34 [1.12-1.61], p=0.001) compared with MBPover90 group (97.3±5.2 mmHg). When stratified by quartiles of baseline cystatin C glomerular filtration ratio (GFR), the association between MBPbelow90 and postoperative AKI remained significant only with the lowest quartile (cystatin C GFR ≤85 mL/min/1.73 m²; IPTW-OR 2.24 [1.53-3.28], p<0.001), but not with 2nd-4th quartiles. CONCLUSIONS Our results suggest that maintaining supranormal MBP over 90 mmHg may be beneficial to reduce the risk of post-LT AKI, especially for liver transplant recipients with cystatin C GFR ≤85 mL/min/1.73 m².
随着终末期肝病的进展,由于自身调节功能受损,肾血流量与平均动脉血压(MBP)呈线性相关。我们研究了术后较低程度的MBP是否能预测肝移植术后急性肾损伤(AKI)的发生。材料与方法:本回顾性研究纳入了1136例术前肾功能正常的受者。根据术后平均MBP将患者分为两组:<90 mmHg(MBP低于90组)和≥90 mmHg(MBP高于90组)。主要终点是术后AKI的发生,根据改善全球肾脏病预后组织的肌酐标准进行定义。采用倾向评分的逆概率处理加权(IPTW)逻辑回归模型比较两组术后AKI的风险。结果:与MBP高于90组(97.3±5.2 mmHg)相比,MBP低于90组(83.0±5.1 mmHg)术后AKI的患病率和风险更高(74.2%对62.6%,p<0.001;IPTW比值比1.34[1.12 - 1.61],p = 0.001)。按基线胱抑素C肾小球滤过率(GFR)四分位数分层时,MBP低于90与术后AKI之间的关联仅在最低四分位数(胱抑素C GFR≤85 mL/min/1.73 m²;IPTW比值比2.24[1.53 - 3.28],p<0.001)时有统计学意义,而在第2 - 4四分位数时无统计学意义。结论:我们的结果表明,维持超过90 mmHg的超常MBP可能有利于降低肝移植术后AKI的风险,尤其是对于胱抑素C GFR≤85 mL/min/1.73 m²的肝移植受者。