Leslie Hannah H, Malata Address, Ndiaye Youssoupha, Kruk Margaret E
Department of Global Health and Population, Harvard TH Chan School of Public Health, Boston, Massachusetts, USA.
Kamuzu College of Nursing, Malawi University of Science and Technology, Limbe, Southern Region, Malawi.
BMJ Glob Health. 2017 Sep 4;2(3):e000424. doi: 10.1136/bmjgh-2017-000424. eCollection 2017.
Measurement of effective coverage (quality-corrected coverage) of essential health services is critical to monitoring progress towards the Sustainable Development Goal for health. We combine facility and household surveys from eight low-income and middle-income countries to examine effective coverage of maternal and child health services.
We developed indices of essential clinical actions for antenatal care, family planning and care for sick children from existing guidelines and used data from direct observations of clinical visits conducted in Haiti, Kenya, Malawi, Namibia, Rwanda, Senegal, Tanzania and Uganda between 2007 and 2015 to measure quality of care delivered. We calculated healthcare coverage for each service from nationally representative household surveys and combined quality with utilisation estimates at the subnational level to quantify effective coverage.
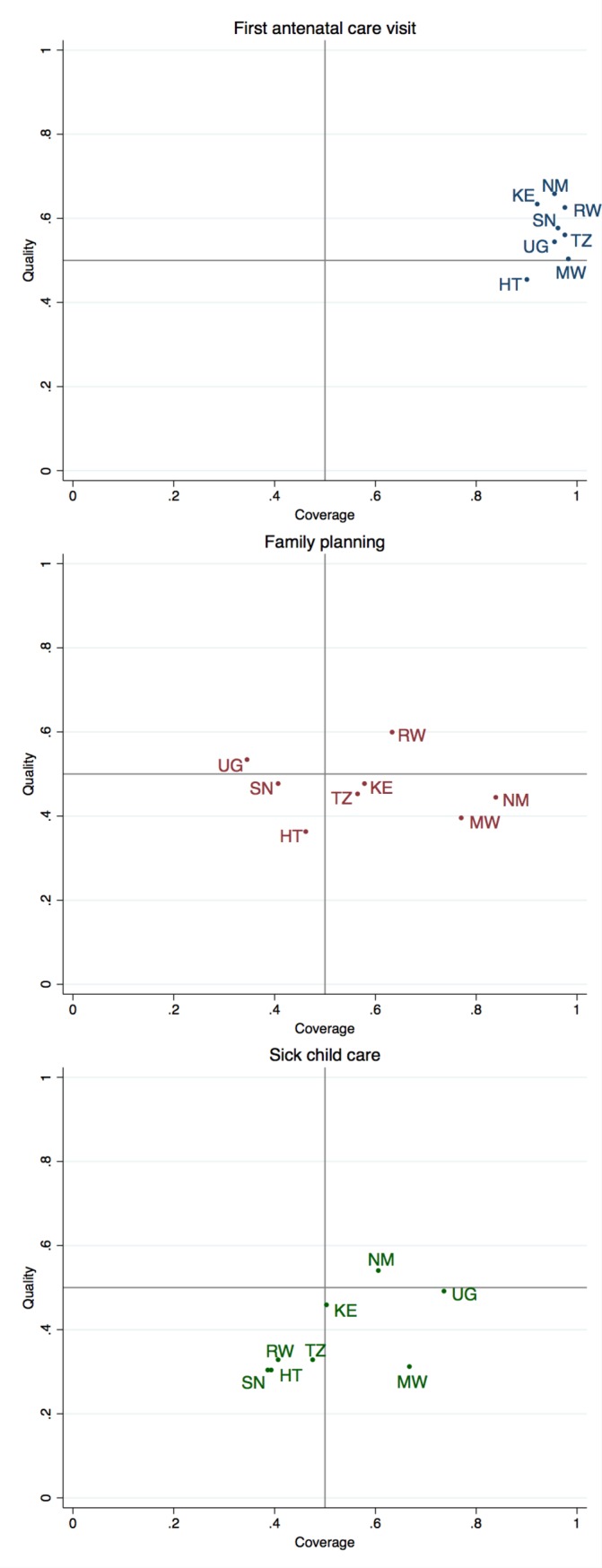
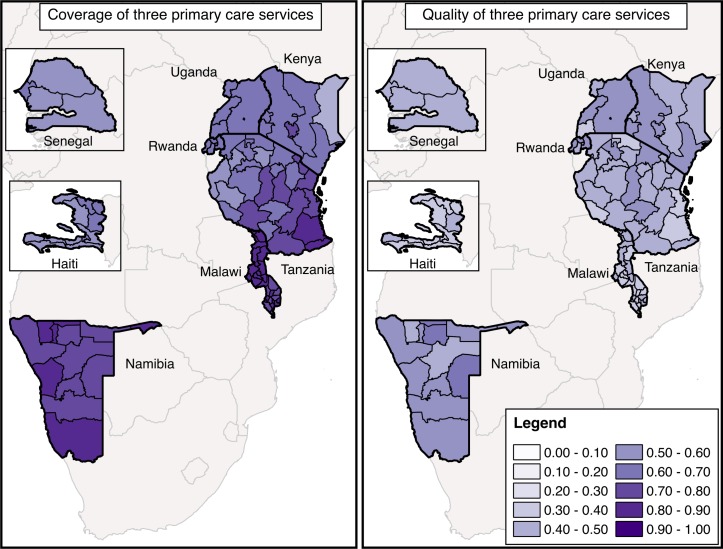
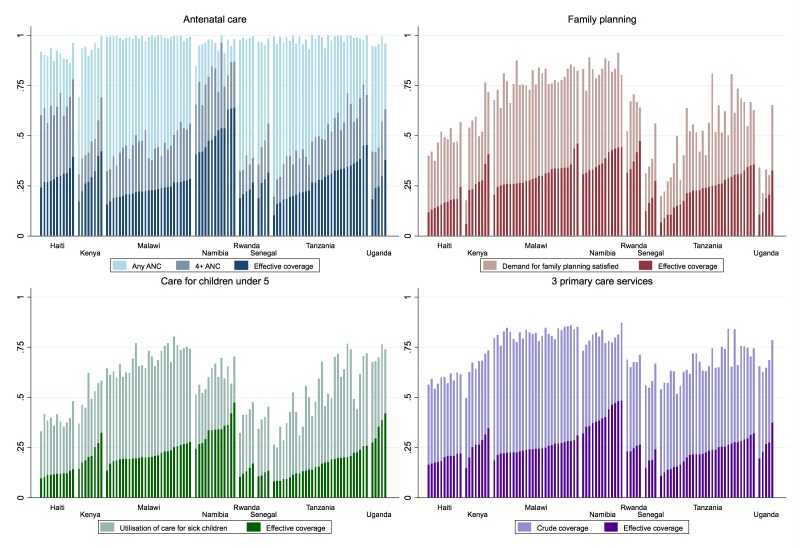
Health facility and household surveys yielded over 40 000 direct clinical observations and over 100 000 individual reports of healthcare utilisation. Coverage varied between services, with much greater use of any antenatal care than family planning or sick-child care, as well as within countries. Quality of care was poor, with few regions demonstrating more than 60% average performance of basic clinical practices in any service. Effective coverage across all eight countries averaged 28% for antenatal care, 26% for family planning and 21% for sick-child care. Coverage and quality were not strongly correlated at the subnational level; effective coverage varied by as much as 20% between regions within a country.
Effective coverage of three primary care services for women and children in eight countries was substantially lower than crude service coverage due to major deficiencies in care quality. Better performing regions can serve as examples for improvement. Systematic increases in the quality of care delivered-not just utilisation gains-will be necessary to progress towards truly beneficial universal health coverage.
衡量基本卫生服务的有效覆盖率(质量校正覆盖率)对于监测实现卫生领域可持续发展目标的进展情况至关重要。我们整合了来自八个低收入和中等收入国家的机构调查与家庭调查,以研究孕产妇和儿童卫生服务的有效覆盖率。
我们根据现有指南制定了产前保健、计划生育和患病儿童护理的基本临床行动指标,并利用2007年至2015年间在海地、肯尼亚、马拉维、纳米比亚、卢旺达、塞内加尔、坦桑尼亚和乌干达进行的临床就诊直接观察数据来衡量所提供护理的质量。我们从具有全国代表性的家庭调查中计算每项服务的医疗保健覆盖率,并将质量与国家以下层面的利用估计值相结合,以量化有效覆盖率。
卫生机构和家庭调查产生了超过40000次直接临床观察以及超过100000份医疗保健利用的个人报告。各项服务的覆盖率各不相同,任何产前保健的使用都比计划生育或患病儿童护理多得多,而且在不同国家之间也存在差异。护理质量较差,很少有地区在任何一项服务中基本临床实践的平均表现超过60%。八个国家的产前保健有效覆盖率平均为28%,计划生育为26%,患病儿童护理为21%。在国家以下层面,覆盖率和质量之间没有很强的相关性;一个国家内不同地区的有效覆盖率差异高达20%。
由于护理质量存在重大缺陷,八个国家针对妇女和儿童的三项初级保健服务的有效覆盖率大大低于粗略的服务覆盖率。表现较好的地区可以作为改进的范例。要朝着真正有益的全民健康覆盖取得进展,不仅要提高利用率,还必须系统性地提高所提供护理的质量。