Kumar Jayant, Reccia Isabella, Sodergren Mikael H, Kusano Tomokazu, Zanellato Artur, Pai Madhava, Spalding Duncan, Zacharoulis Dimitris, Habib Nagy
Department of Surgery and Cancer, Hammersmith Campus, Imperial College London, London, UK.
Department of General Surgery, University Hospital of Larissa, Larissa, Greece.
Oncotarget. 2018 Feb 28;9(21):15732-15739. doi: 10.18632/oncotarget.24596. eCollection 2018 Mar 20.
Despite careful patient selection and preoperative investigations curative resection rate (R0) in pancreaticoduodenectomy ranges from 15% to 87%. Here we describe a new palliative approach for pancreaticoduodenectomy using a radiofrequency energy device to ablate tumor in patients undergoing R1/R2 resections for locally advanced pancreatic ductal adenocarcinoma where vascular reconstruction was not feasible.
There was neither postoperative mortality nor significant morbidity. Each time the ablation lasted less than 15 minutes. Following radiofrequency ablation it was observed that the tumor remnant attached to the vessel had shrunk significantly. In four patients this allowed easier separation and dissection of the ablated tumor from the adherent vessel leading to R1 resection. In the other two patients, the ablated tumor did not separate from vessel due to true tumor invasion and patients had an R2 resection. The ablated remnant part of the tumor was left
Whenever pancreaticoduodenectomy with R0 resection cannot be achieved, this new palliative procedure could be considered in order to facilitate resection and enable maximum destruction in remnant tumors.
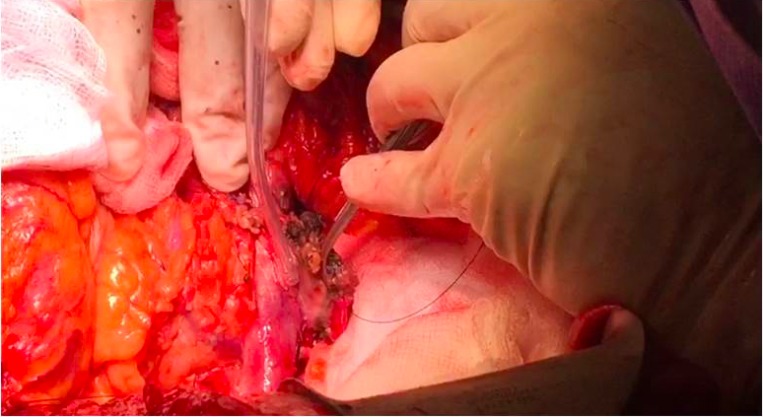
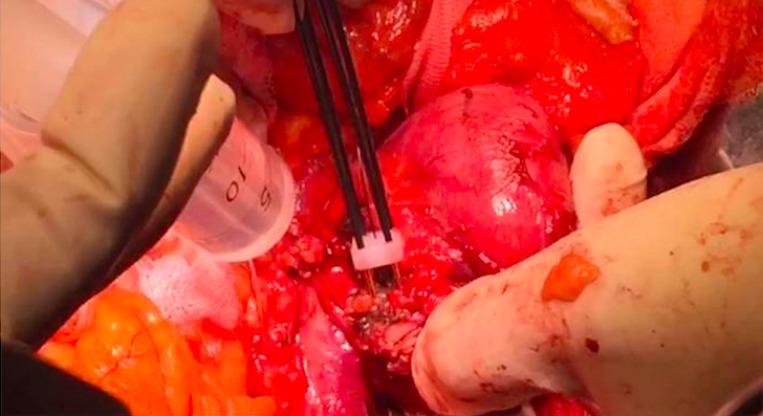
Six patients with suspected tumor infiltration and where vascular reconstruction was not warranted underwent radiofrequency-assisted pancreaticoduodenectomy for locally advanced pancreatic ductal adenocarcinoma. Radiofrequency was applied across the tumor vertically 5-10 mm from the edge of the mesenteric and portal veins. Following ablation, the duodenum and the head of pancreas were removed after knife excision along the ablated line. The remaining ablated tissue was left attached to the vessel.
尽管在患者选择和术前检查方面十分谨慎,但胰十二指肠切除术的根治性切除率(R0)仍在15%至87%之间。在此,我们描述一种新的胰十二指肠切除姑息治疗方法,该方法使用射频能量装置对因局部晚期胰腺导管腺癌而行R1/R2切除且无法进行血管重建的患者的肿瘤进行消融。
术后既无死亡病例,也无严重并发症。每次消融持续时间均小于15分钟。射频消融后观察到,附着于血管的肿瘤残余明显缩小。在4例患者中,这使得更容易将消融后的肿瘤与粘连的血管分离并进行解剖,从而实现R1切除。在另外2例患者中,由于肿瘤的真正浸润,消融后的肿瘤未与血管分离,患者接受了R2切除。肿瘤的消融残余部分被保留。
每当无法实现R0切除的胰十二指肠切除术时,可考虑采用这种新的姑息治疗方法,以促进切除并最大程度地破坏残余肿瘤。
6例疑似肿瘤浸润且无需进行血管重建的患者因局部晚期胰腺导管腺癌接受了射频辅助胰十二指肠切除术。射频垂直于肿瘤,在距肠系膜静脉和门静脉边缘5-10毫米处施加。消融后,沿消融线用刀切除十二指肠和胰头。剩余的消融组织保留附着于血管。