Department of Ambulatory Care and Community Medicine, University of Lausanne, Lausanne, Switzerland.
Service of Cardiology, Lausanne University Hospital, Lausanne, Switzerland.
PLoS One. 2018 Apr 12;13(4):e0195174. doi: 10.1371/journal.pone.0195174. eCollection 2018.
To examine the prognosis of patients with cardiovascular and non-cardiovascular multimorbidity after acute coronary syndrome compared to patients without prior multimorbidity.
This multicenter prospective cohort study in Switzerland included 5,635 patients hospitalized with acute coronary syndrome between 2009 and 2014, with a one-year follow-up period. We defined cardiovascular and non-cardiovascular multimorbidity as having at least two prior comorbidities before the index hospitalization. Multivariable adjusted Cox proportional models were built to assess the one-year risk of recurrent cardiovascular events, defined as cardiovascular mortality and non-fatal myocardial infarction or stroke. The final model was adjusted for age, gender, body mass index, tobacco consumption, education, and family history of cardiovascular disease, prescription of high-dose statinsat discharge and use of cardiac rehabilitation after discharge.
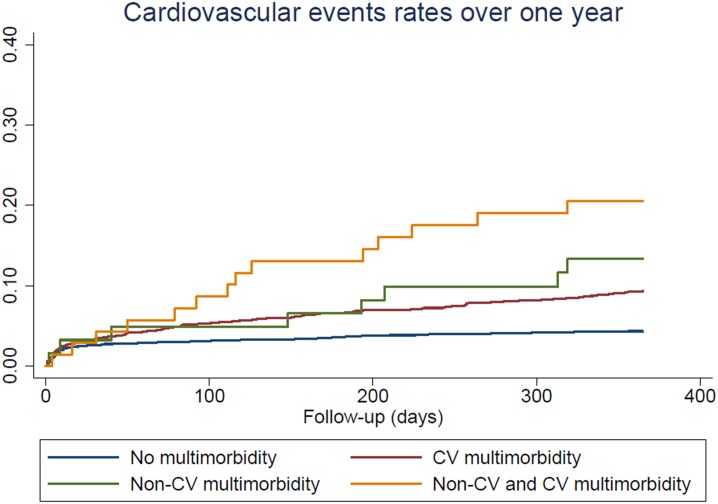
Overall, 3,664 patients (65%) had no multimorbidity, 1,839 (33%) had cardiovascular multimorbidity, 62 (1%) had non-cardiovascular multimorbidity, and 70 (1%) had both cardiovascular and non-cardiovascular multimorbidity. The multivariate risk of recurrent cardiovascular events was increased among patients with cardiovascular multimorbidity (hazard ratio (HR) 2.05, 95% CI: 1.54-2.73, p<0.001) and patients with non-cardiovascular multimorbidity (HR 2.57, 95% CI: 1.04-6.35, p = 0.04) compared to patients without multimorbidity. Patients with cardiovascular and non-cardiovascular multimorbidity had the highest risk of recurrence with a HR of 5.19, 95% CI: 2.79-9.64, p<0.001, compared to patients without multimorbidity.
Multimorbidity increased by two-fold the risk of cardiovascular events over the year after an acute coronary syndrome. The magnitude of this increased risk was similar for patients with cardiovascular or non-cardiovascular multimorbidity.
与无既往多重合并症的患者相比,检查急性冠状动脉综合征后心血管和非心血管多重合并症患者的预后。
本研究在瑞士进行,为一项多中心前瞻性队列研究,共纳入 2009 年至 2014 年期间因急性冠状动脉综合征住院的 5635 例患者,随访 1 年。我们将心血管和非心血管多重合并症定义为在指数住院前至少有两种既往合并症。采用多变量调整 Cox 比例模型评估 1 年内复发性心血管事件的风险,定义为心血管死亡率和非致死性心肌梗死或卒中。最终模型调整了年龄、性别、体重指数、吸烟、教育程度和心血管疾病家族史、出院时高剂量他汀类药物的处方和出院后心脏康复的使用。
总体而言,3664 例(65%)患者无多重合并症,1839 例(33%)患者有心血管多重合并症,62 例(1%)患者有非心血管多重合并症,70 例(1%)患者有心血管和非心血管多重合并症。与无多重合并症的患者相比,有心血管多重合并症的患者(风险比 2.05,95%置信区间:1.54-2.73,p<0.001)和有非心血管多重合并症的患者(风险比 2.57,95%置信区间:1.04-6.35,p = 0.04)复发性心血管事件的风险增加。与无多重合并症的患者相比,有心血管和非心血管多重合并症的患者复发风险最高,风险比为 5.19,95%置信区间:2.79-9.64,p<0.001。
急性冠状动脉综合征后 1 年内,多重合并症使心血管事件的风险增加了一倍。心血管或非心血管多重合并症患者的这种风险增加幅度相似。